
Abstract
Objective
We report on the use of portable computed tomography (CT) in an ICU setting. The additional diagnostic gain and therapeutic consequences were assessed.
Patients
Ten ICU patients underwent 14 portable chest CT examinations. In 64% maximum intensive care was required, according to TISS28 (>40), and 42% were at a risk of mortality higher than 25% (MODS) on the day of portable CT examination. In three portable CT examinations the patients were considered not transportable and were examined directly in the patient room. All other examinations were performed in a special interventional suite directly on the ICU.
Results
Of 14 examinations 8 (57%) resulted in a change in patient management within 48 h. All patients profited from portable CT and no hazards occurred related to CT.
Conclusions
To perform portable CT in the interventional suite on the ICU allows immediate minimally invasive therapeutic interventions and provides full ICU monitoring.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
With advances in technology, critically ill patients increasingly require intrahospital transport for diagnostic testing. Among these tests computed tomography (CT) is one of the most frequently employed [1, 2]. Most intensivists would accept that it is better to bring a diagnostic device to a critically ill patient than vice versa. Because of the well documented hazards and expenses of transfer and its unfeasibility for some critically ill patients, the ICU or even the bedside is an appealing site for diagnostic procedures [3, 4, 5, 6]. On our ICU we apply two different approaches with regard to the use of the portable CT scanner. One is a bedside method suitable for ICU patients who cannot be transported at all. Alternatively, there is a special interventional suite directly on the ICU where portable CT can be performed thereby offering full ICU monitoring.
Here we report our experience with portable CT which we have employed for a 1 year period in the medical and surgical ICU of our tertiary care center. The aim of this study is to introduce the portable CT technology in ICU settings. It is presented as an addition to the other available diagnostic tools the object of which is an advanced use of diagnostic imaging (AUDI) locally on the ICU.
Material and methods
Patients
Only patients with chest CT examination were included. The CT results were compared with simultaneously performed plain chest radiographs. Ten patients underwent 14 chest CT examinations performed with portable CT in our tertiary care ICU during a 1-year period. The study included four women and six men; the average age was 56 years (range 31–82 years). For better characterization of ICU patients, they were analyzed retrospectively by scores—Acute Physiology and Chronic Health Evaluation II (APACHE II) [7], Multiple-Organ Dysfunction Score (MODS) [8], and Therapeutic Intervention Scoring System 28 (TISS 28) [9] and by the judgment by an intensivist.
Clinical environment
The interventional suite is a specially equipped 35 m2 room located in the center of the ICU that can be easily reached from all patient rooms. It was designed to perform interventional and diagnostic procedures (e.g., ultrasound, fluoroscopy, and endoscopy) within the ICU (Fig. 1).

Portable CT located in the interventional suite directly in on the ICU
Technical equipment
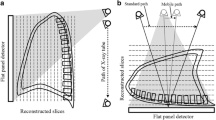
The portable spiral CT scanner (Tomoscan M, Philips, Eindhoven, The Netherlands) was used. It consists of three components (gantry, CT table, and workstation) the pieces of which can be unplugged and transported separately (Fig. 2). This CT system is accumulator driven, allowing several scans in succession without recharging. The rotation time is 2 s, maximum scan area is 65 cm with a pitch of 2 (table travel of 10 mm per rotation and a slice thickness of 5 mm). The term pitch describes the ratio of table travel per rotation of the detector system inside the gantry to the slice thickness chosen. The gantry offers an independent horizontal movement of 35 cm relative to its chassis which permits the performance of head CT as a bedside method without moving the patient from bed.

Portable CT performed directly in the patient rooms
Clinical evaluation
Indications for portable CT were theorized, and indication grades were ranked according to a scale ranging from 1 (essential) to 5 (not indicated):
-
1.
Essential: CT is absolutely indicated and must be performed at once
-
2.
Necessary: CT is important for diagnosis of disease
-
3.
Moderate: CT could reveal some new information and could eventually be performed later
-
4.
Not obvious: CT is elective
-
5.
Not indicated: CT is senseless
Furthermore the diagnostic gain of CT examination was compared to portable plain chest radiographs. Additionally, for exact determination of diagnostic value of portable CT the changes in therapeutic management were noted.
Results
All patients had intra-arterial pressure monitoring and were connected to a portable electrocardiography monitor and pulse-oxymeter throughout the period of transport to the interventional suite and CT examination. All essential medications were continued with battery-operated perfusor pumps without interruption. For patients examined in the interventional suite the ventilation was usually maintained by means of a portable ventilator (Servo 900, Erlangen, Siemens, Germany, or Oxylog Emergency Ventilator, Dräger, Lübeck, Germany) during transport. Otherwise, advanced ventilation with high-quality devices was provided during CT examination.
Three scans were performed as bedside examinations in the patient room and 11 in the interventional suite on the ICU. Patient characteristics, indications for CT, scores, assessment of transportability, and retrospective analysis of consequences are listed in Table 1. No significant hemodynamic or respiratory deterioration or any other notable mishap was observed which could have been attributed to the use of portable CT and the transfer to the interventional suite. Eight of the 14 examinations resulted in a change in patient management within 48 h. The ranges of scores for APACHE II, TISS 28, and MODS were 17–39, 29–52, and 3–18, respectively. Three patients were judged by an intensivist to be not transportable and were therefore examined in the patient room directly. Of 14 chest CT examinations five were performed on admission to the ICU in the patient room or the interventional suite.
Compared to plain chest radiographs, portable CT demonstrated a gain of additional diagnostic information in 9 of 14 cases. There were direct changes in therapy in 8 patients. In 4 patients an interventional procedure such as chest drainage was applied, and two patients were operated upon immediately after the portable CT scanning.
Discussion
The portable CT scanner can be used in a flexible manner in hospital [10, 11, 12]. In this report we describe its use for chest CT in the ICU. First, we employed the portable CT scanner in a specially designed interventional suite. On the one hand, this approach offers the advantages of full monitoring and ventilation with modern ICU ventilators using the same method as in the patient room. On the other hand, there is still the disadvantage of moving the patient to the diagnostic device instead of vice versa. Although the portability of the CT scanner used is not applied in this way, the distances and durations of transports inside the ICU are much less than those to the radiology department. Another advantage of this method is the continued availability of the intensivist on the ICU, who otherwise had to accompany the patient during transport. A possible time advantage in using the portable CT scanner in the interventional suite is limited by its technical capabilities. Both planning the examination and acquiring the data by the portable CT scanner take clearly longer than CT in the radiology department. Taking everything into account, a portable CT scanner on the ICU offers continued intensive care monitoring during examination with the equivalent overall time consumption as the CT examination in the radiology department.
Second, only if transport would be too hazardous or impossible at all a bedside CT examination was performed. This was the case in three of ten patients. This approach was rather time and effort consuming. This was not only stimulated by the method itself but also by the underlying diagnosis of examined patients. For those patients a bedside examination was the only option for CT. Performing such a diagnostic procedure in the patient's room was expensive because of the need for many additional aides (transportation of devices, transfer of the patient from bed to CT table) and the factor of time consumption. The latter was an important consideration because the performing of CT in patients' rooms was not provided for at the time of their construction. First, there had to be an evaluation of safety according to the guidelines of German radiation protection. The indication for CT was carefully assessed following these guidelines. Other patients in such a room had to be removed, and neighboring rooms had to be shielded by portable walls made of lead.
Although these CT examinations yielded additional diagnostic information compared to conventional radiography, and although changes in therapeutic procedures were made according to these additional findings, all patients finally died at the end of their intensive care treatment. Regardless of the outcome with regard to particular patients, use of the portable CT yielded valuable, otherwise unavailable diagnostic information. Portable CT findings prompted a change in patient management in eight patients, a relatively high proportion. This figure underscores the value of images performed by portable CT. The reasonable quality of images obtained by portable CT is also reported in the literature [13, 14]. On the other hand, a specially trained radiology team is required which should be available 24 h a day, 7 days a week. The work load for the radiology department and staffing costs will increase. Hence the routine use of portable CT which serves only for very selected patients seems economically feasible only for large medical centers with a shared use of this device in the operating theater, emergency room, and ICU.
It seems that portable CT is best reserved for neurosurgical ICU patients. Gunnarsson et al. [15] report the use of the gantry only in neurosurgical ICU settings. They arranged the patients with their heads pointing to the middle of the patient rooms. This position allows easy access for the gantry able to move horizontally for rapidly performed head CT. Our study demonstrated that portable CT provides significant diagnostic gain over plain chest radiography. No hazards occurred in our patients during portable CT. Portable CT provides full ICU monitoring when performed in the interventional suite directly on the ICU.
References
Gartenschläger M, Schweden F, Dueber C, Weilemann LS, Westermeier T, Thelen M (1998) Klinische Relevanz der Thorax-CT in Intensiv- und Notfallmedizin. Aktuelle Radiol 8:260–265
Miller WT Jr, Tino G, Friedburg JS (1998) Thoracic CT in the intensive care unit: assessment of clinical usefulness. Radiology 209:491–498
Braxton CC, Reilly PM, Schwab CW (2000) The traveling intensive care unit patient. Road trips. Surg Clin North Am 80:949–956
Szem JW, Hydo LJ, Fischer E, Kapur S, Klemperer J, Barie PS (1995) High-risk intrahospital transport of critically ill patients: safety and outcome of the necessary "road trip." Crit Care Med 23:1660–1666
Waydhas C (1999) Intrahospital transport of critically ill patients. Crit Care 3:83–89
Rückoldt H, Marx G, Leuwer M, Panning B, Piepenbrock S (1998) Pulsoxymetrie und Kapnometrie bei Intensivtransporten: kombinierter Einsatz verringert das Transportrisiko. Anasthesiol Intensivmed Notfallmed Schmerzther 32:32–36
Knaus WA, Draper EA, Wagner DP, Zimmermann JE (1985) APACHE II: a severity of disease classification system. Crit Care Med 13:818–829
Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, Sibbald WJ (1995) Multiple Organ Dysfunction Score: a reliable descriptor of a complex clinical outcome. Crit Care Med 23:1638–1652
Miranda DR, de Rijk A, Schaufeli W (1996) Simplified Therapeutic Intervention Scoring System: the TISS-28 items—results from a multicenter study Crit Care Med 24:54–73
White CS, Meyer CA, Wu J, Mirvis SE (1999) Portable CT: assesing thoracic disease in the intensive care unit. AJR Am J Radiol 173:1351–1356
Butler WE, Piaggio C, Constantinou C, Niklason L, Gonzalez GR, Cosgrove RG, Zervas NT (1998) A mobile computed tomographic scanner with intraoperative and intensive care unit applications. Neurosurgery 42:1304–1311
Dowd MT, Hathaway PB, Fontaine AB, Borsa JJ, Nelson M, Hoffer E (1999) Combined use of mobile CT and fluoroscopy in the angiography suite. AJR Am J Radiol 172:497–498
Matson MB, Jarosz JM, Gallacher D, Malcolm PN, Holemans JA, Leong C, Seed PT, Ayers AB, Rankin SC (1999) Evaluation of head examinations produced with a mobile CT unit. Br J Radiol 72:631–636
Mirvis S, Shanmuganathan K, Donohue R (1997) Mobile computed tomography in the trauma/critical care environment: preliminary clinical experience. Emerg Radiol 4:1–6
Gunnarsson T, Theodorsson A, Karlsson P, Fridriksson S, Bostroem S, Persliden J, Johansson I, Hillman J (2000) Mobile computerized tomography scanning in the neurosurgery intensive care unit: increase in patient safety and reduction of staff workload. J Neurosurg 93:432–436
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Teichgräber, U.K.M., Pinkernelle, J., Jürgensen, JS. et al. Portable computed tomography performed on the intensive care unit. Intensive Care Med 29, 491–495 (2003). https://doi.org/10.1007/s00134-002-1606-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-002-1606-x