
Abstract
Aims/hypothesis
Young adults in the early stages of their participation in the labour market may be particularly vulnerable to the effects of onset of a chronic disease. Our aim was to quantify the consequences of the onset of type 1 diabetes in young adults on annual earnings, using individual-level longitudinal data before and after the onset of diabetes.
Methods
The Econ-DISS database contains annual socioeconomic information for 1990–2005 from Statistics Sweden. Econ-DISS includes data for persons with diabetes onset at the age of 15–34 years between 1983 and 2005, registered in the national Diabetes Incidence Study in Sweden (DISS) database, and for controls. Considering the onset of type 1 diabetes as an unanticipated and significant life event, we compared the progression of annual earnings for 3,650 cases born between 1949 and 1970 before and after onset of diabetes with that of 14,629 controls. Possible confounders—education, participation in the labour market, sick leave and parental education—were analysed.
Results
We found no differences between the groups in annual earnings or participation in the labour market before onset of diabetes. After onset, persons with type 1 diabetes gradually lagged behind the controls. Their median annual earnings were lower in each year from 1995 to 2005 (p < 0.01). The difference in 2005 was euro (EUR) 1,411 (5.3%). Controlling for confounders, duration of type 1 diabetes ≥10 years was associated with 4.2% (men) and 8.1% (women) lower average annual earnings for persons with upper secondary education only who were active in the labour market.
Conclusion/interpretation
The onset of type 1 diabetes in young adults has long-term detrimental consequences on earnings that cannot be attributed to confounders.
Similar content being viewed by others


Introduction
Young adults at a stage of life in which they choose education, and enter and become established in the labour market, might be particularly vulnerable to the impact of the onset of a chronic disease. The scarce literature on consequences of type 1 diabetes on earnings, education and participation in the labour market may be explained by the difficulties in obtaining data to confirm a causal relationship. A few published studies have described labour-market outcomes for persons with diabetes of varying duration, relying on cross-sectional data and on self-reporting of diabetes in surveys [1–12]. Cross-sectional data may show associations, but are not sufficient for identifying causal relationships. For instance, analyses of the economics of the labour force have shown a substantial association between parental socioeconomic status and children’s lifetime earnings [13–15]. In addition, surveys do not always distinguish between type 1 and type 2 diabetes, for which one might expect differences in the impact on labour-market outcomes.
We analysed the development of the annual distribution of earnings in 1990–2005 comparing a cohort of individuals who were 15–34 years old at the onset of type 1 diabetes with a control group from the Swedish population. Using individual-level data on longitudinal earnings from high-quality public administrative registries before and after the onset of diabetes, we accounted for potential confounding factors: education, employment, and socioeconomic status measured by parents’ level of education.
Methods
The Econ-DISS research database
Econ-DISS was designed to study the consequences of the onset of diabetes in early adulthood for labour-market outcomes, including earnings, education, participation in the labour market and use of social insurance. It is based on the national Diabetes Incidence Study in Sweden (DISS) database [16], which is a register of incident cases of diabetes in young adults aged 15–34 years old (about 400 per year) since 1983 [17, 18]. Participants were classified by the reporting physician according to clinical criteria established by WHO [19, 20] during the first period 1983–1991 [21]. Since 1992 the diagnostic criteria used [18] are those recommended by the American Diabetes Association expert group [22], in clinical settings corresponding to those of WHO [23]. The clinical classification has been shown to correspond well to the presence of islet cell antibodies and C-peptide concentrations [24, 25]. For the period 1983–2005, 73% of individuals were registered as having type 1 diabetes, 17% as having type 2 diabetes and 10% were unclassifiable at the time of diagnosis. Statistics Sweden [26] selected for each case in DISS four control persons matched by age, sex and municipality of residence at the time of diabetes diagnosis. In addition, parents of cases and controls were identified using the Multiple Generations Register at Statistics Sweden.
The Econ-DISS population consists of 9,298 young adults with diabetes onset between 1983 and 2005 in Sweden and 37,192 controls. For this study, we selected all individuals born in 1949–1970 and registered with type 1 diabetes onset at ages 15–34 years during the years 1983–2005 (n = 3,650), and their controls (n = 14,629). In 1990, the first year of earnings data, the youngest individuals were 20 years old and potentially active in the labour market.
The Econ-DISS longitudinal database contains individual-level annual data for 1990–2005 on 290 demographic, socioeconomic and employer-related variables from the Longitudinal Integration Database for Health Insurance and Labour Market Studies (LISA) at Statistics Sweden, which covers the entire population in Sweden aged ≥16 years [27]. All information was linked at the individual level by Statistics Sweden using the civic registration number. The research programme was approved by the Regional Ethical Review Board in Lund, Sweden (dnr 393/2005).
Exposure
Our exposure was diabetes onset at ages 15–34 years. Controls were expected to reflect the general population.
Analyses of the development of earnings
We analysed the annual distributions of earnings and of the confounders, achieved level of education, participation in the labour market (employment status, unemployment benefits, days of unemployment, periods of sick leave) and parents’ level of education prior to the onset of type 1 diabetes (see Electronic supplementary material [ESM] Table 1). Disparities in earnings and confounders before onset would reduce the degree of differences in earnings after onset that could be attributed to diabetes per se.
We followed the birth cohorts 1949–1970 from 1990 to 2005 using two overall groupings: before/after onset and diabetes/control group. By design, the number of persons in the ‘before diabetes onset group’ decreased over time and, correspondingly, the number increased in the ‘after diabetes onset group’ (ESM Table 2).
Earnings data were analysed in three ways. First, we analysed whether the distribution of earnings differed between cases and controls in any single year in 1990–2005. Second, we analysed the earnings of cases relative to the average earnings of their respective controls, organising data by duration of diabetes. Finally, the impact of diabetes and disease duration on the 4-year average annual earnings in 2002–2005 (smoothing transitory fluctuations) were analysed, controlling for confounders in a standard labour-economic model [28]. Models were estimated in the full sample (model 1) and in a restricted sample comprising persons active in the labour market in all years in 2002–2005 (model 2). The models used interactions of diabetes duration and education to capture potential educational gradients on the effects of diabetes on earnings. Earnings were measured in Swedish kronas (SEK) to avoid exchange-rate-driven fluctuations. Key results were converted to EUR [29].
Statistical methods
Non-parametric Pearson χ 2 test of median values was used for comparison of continuous variables (earnings, days of unemployment and sick leave). For single years, binary and categorical variables were compared using χ 2 test and test of proportion [30]. Pooling observations in 1990–2005, ORs with 95% CI for binary variables were obtained by logistic regression accounting for intra-individual correlation using cluster option for standard errors and controls as reference category [31]. The individuals’ levels of education, adjusted for maternal and paternal level of education, respectively, were analysed using the Mantel–Haenszel method [30]. Non-parametric kernel density estimation was used to estimate smooth density functions of earnings [31]. Logistic regression analysis was used to analyse the probability of not being in the labour market in the years 2002–2005 [30]. Semi-logarithmic ordinary least squares analysis was used to analyse average annual earnings in 2002–2005 [28, 32]. Stata version 10.1 was used for the statistical analyses (www.stata.com) [31].
Results
Annual earnings
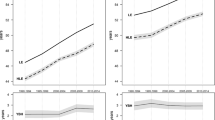
Figure 1 shows the development of first, second (median) and third quartiles of annual earnings in 1990–2000 in the before-onset group. We found no significant differences in median earnings. Figure 2 shows the development of earnings including individuals from the year of onset of diabetes. The median earnings of cases and controls were different (p < 0.01) each year in 1995–2005. In 2005, the difference in median earnings was SEK 13,100 (EUR 1,411), corresponding to 5.3% lower earnings for persons with type 1 diabetes. The difference was greater for persons with the lowest earnings (first quartile): SEK 25,200 (EUR 2,714; 18%). Earnings differentials were of similar magnitude when the first 2 years of diabetes from the after-onset group were excluded.

Development of annual earnings for diabetes (dashed line, white circles) and control group (solid line, black circles) before the onset of diabetes. First (Q1), second (Q2, median) and third (Q3) quartiles of annual earnings 1990–2000

Development of annual earnings for diabetes (dashed line, white circles) and control group (solid line, black circles) after the onset of diabetes. First (Q1), second (Q2, median) and third (Q3) quartiles of annual earnings 1990–2005
The onset of type 1 diabetes was associated with a marked decline in earnings compared with the background population (Fig. 3). The relative earnings before onset varied randomly. In the year of onset, the median ratio of earnings by cases to the average earnings by his/her controls was 102.1%. Ten years after onset, the cases earned 4.0% less and after 20 years, 10% less.

Median relative earnings: the earnings of cases as percentage of the mean earnings of his/her controls before and after onset, with number of persons in diabetes group within parentheses. Year of onset: 102.1%; year 10: 96%; year 20: 89.7%
Before onset: analyses of education, participation in the labour market and sick leave
We found no differences in employment (OR 1.07, 95% CI 0.95–1.19), receipt of unemployment benefits (OR 1.07, 95% CI 0.95–1.20) or having at least one period of sick days (OR 1.08, 95% CI 0.92–1.27), pooling data from the years 1990–2000 (reference controls = 1.00; ESM Figs 1, 2). In addition, we did not find differences in annual proportions for the same variables. Length of sick leave and unemployment did not differ, except for unemployment in 1999.
There was a tendency towards difference in educational achievement: compulsory education only (OR 1.18, 95% CI 0.99–1.41) and in university education (OR 0.86, 95% CI 0.73–1.00; ESM Fig. 3). In 1990, the percentage of persons with compulsory education only was 19% in the diabetes group and 17% in control group (p < 0.05). The corresponding figures for university education were 14% and 16% (p < 0.05). Adjusting for paternal level of education, the Mantel–Haenszel ORs were 1.20 (95% CI 1.03–1.40) for own compulsory education only and 0.82 (95% CI 0.69–0.97) for university. There were no significant differences in proportions in each single year after 1990.
Overall, parents of persons with diabetes were slightly more likely to have completed compulsory education only (Table 1). Annual earnings in subgroups by parents’ level of education did not differ before onset of diabetes, with the exception that cases where mothers had completed upper secondary education only had higher earnings than controls in 1990.
After onset: differences in factors associated with earnings
Cases were more likely to be without employment (OR 1.14, 95% CI 1.06–1.21), and a higher percentage received unemployment benefits in six of 16 years. Cases were more likely to have had at least one period of sick leave (OR 1.53, 95% CI 1.45–1.61), and a higher percentage had sick leave in 13 of 13 years (p < 0.001, all years; ESM Figs 1, 2).
The annual percentage of persons in the diabetes group with university education was significantly lower for all years and, correspondingly, higher for compulsory education only in seven of 16 years. The OR from pooled data in 1990–2005 was 1.11 (95% CI 1.01–1.22) for compulsory education only and 0.88 (95% CI 0.81–0.95) for university (ESM Fig. 3). By subgroups of parental education (Table 1), earnings differentials between individuals were predominantly found where parents had completed compulsory education only, but also where parents had completed upper secondary education.
Diabetes, employment and average annual earnings in 2002–2005
The diabetes group were over-represented among persons with low earnings (Fig. 4a, full sample, and Fig. 4b, sample active in the labour market all 4 years 2002–2005; 77%). Both groups had persons without earnings in at least 1 year, as shown by the bimodal densities (Fig. 4a).

Kernel density estimate for average annual earnings 2002–2005 for diabetes (dashed line, white circles) and control group (solid line, black circles) (a) Full sample (N = 17,227) and average annual earnings below SEK 800,000 (EUR 86,161 [29]). Estimated by Epanechnikov kernel function and the Stata default half-width of the kernel: 2.4 for cases and 1.8 for controls [31]. (b) Sample active in the labour market all 4 years (n = 13,290) and average annual earnings below SEK 800,000 (EUR 86,161 [29]). Estimated by Epanechnikov kernel function and Stata default half-width of the kernel: 1.7 for cases and 1.4 for controls [31]
We found significant associations between diabetes, employment and average annual earnings in 2002–2005 in the multiple regression analyses, estimated separately for men and women, and controlling for age, living in major urban area, and own and parental education. Women with diabetes duration ≥10 years and compulsory education only were less likely to be employed (OR 1.72, 95% CI 1.12–2.64), all else being equal (Table 2; full results in ESM Table 3).
Table 3 presents the percentage effect of diabetes on earnings by level of education for men and women, controlling for confounders (full results in ESM Table 4). Model 1 was estimated in the full samples of men and of women, respectively. Diabetes duration ≥10 years had a negative impact on earnings for persons with compulsory education only and with upper secondary education only (men with compulsory education only −36% [p = 0.03] and upper secondary education only −24% [p < 0.01]; women with only education −41% [p < 0.01]). There was a strong counteracting effect of university education for women with diabetes duration ≥10 years, and the joint effect was +17% (p = 0.03).
Model 2 was estimated in the subsample active in the labour market all 4 years in 2002–2005 (men 78%; women 74%). There was a negative effect on earnings for women with compulsory and upper secondary education only (7% and 53% of women with diabetes, respectively) and diabetes duration 1–9 years. Diabetes duration ≥10 years was associated with a negative effect on earnings for men (−4.2%) and women (−8.1%) with upper secondary education only (Table 3, model 2).
Discussion
We analysed the development of annual earnings in 1990–2005 for persons with type 1 diabetes onset at ages 15–34 years compared with persons of the same age, sex and municipality of residence. We found no differences in earnings before the onset of diabetes, but a trend of increasing earnings differentials after onset (Figs 2 and 3).
Previous studies from Canada and the USA have indicated differences in earnings, but did not consider type 1 diabetes in particular, nor did they control for duration of diabetes [1–12]. In this study we have established more firmly, first, that the differences in earnings were in fact induced by the onset of diabetes using the before–after design and individual-level longitudinal annual data. Second, after onset, women with compulsory education only and diabetes duration ≥10 years were more likely to be unemployed (Table 2); among persons active in the labour market (Fig. 4b and Table 3, model 2), we found negative effects on earnings for women with compulsory and with upper secondary education only. Diabetes duration ≥10 years was associated with persistent lower earnings for women with upper secondary education only (−8.1%), and in addition for men with upper secondary education only (−4.2%), when controlling for confounders. Future analyses will address whether this result may be explained by lower wages, less time worked or the choice of sector of the labour market. Third, cases were more likely to have at least one period of sick leave (ESM Fig. 2), but the total number of days of sick leave during the year did not differ in 10 of 13 years for cases and controls with positive sickness absence.
A strength of our analysis was the design using observational longitudinal labour-market data before and after the onset of type 1 diabetes. This may resemble a randomised natural experiment of the effect of changes in health on labour-market outcome. The onset of diabetes requires a change in daily life habits in which the person must devote time to preventive treatment and to the care of diabetes-related events and complications. The Econ-DISS data showed a marked decline in earnings at onset (Fig. 3) and consistently lower earnings, even before the time when complications of diabetes would be expected to arise.
The analogy of a randomised experiment with respect to labour-market outcome is based on two assumptions: that individuals (1) do not by their actions influence the onset of type 1 diabetes, and (2) have no reason to anticipate the onset. We believe that the assumptions hold reasonably well for type 1 diabetes. The onset of type 1 diabetes is almost always sudden and unanticipated. Moreover, only a minority of people with diabetes has relatives with diabetes [33, 34] and only one of 15 in the general population with the highest risk HLA genotype will eventually develop type 1 diabetes [35]. Thus, as observed in this study, we did not expect systematic differences in labour-market behaviour between cases and controls prior to diabetes onset. We also propose that the observed lower earnings after onset may be considered a consequence of type 1 diabetes.
However, a potential weakness in the study design was the assumption of no differences prior to onset of diabetes, as two studies have pointed to a possible association between socioeconomic status and the incidence of childhood onset of type 1 diabetes [36, 37]. Parental human capital is also associated with their children’s labour-market outcomes [13, 14], and crude comparisons would then overstate the pure diabetes-related effect on earnings. We found a slight over-representation of parents with only compulsory education in the diabetes group (Table 1). However, we were able to control for parental level of education in the regression analyses on employment and earnings, using Econ-DISS. We found only weak evidence of effects of parental education (ESM Tables 3, 4). Analyses of earnings after onset showed that median annual earnings differed within subgroups by parental level of education (Table 1). In particular, controls had higher median earnings in the subgroups with maternal and paternal completion of only compulsory education in 15 of 16 years. These findings support the hypothesis that the onset of diabetes has negative effects on earnings, in addition to differences that may be explained by parental education.
During the incident years of Econ-DISS (1983–2005), technological advances, including treatment devices and intensive treatment regimens, have contributed to better glycaemic control in general [38]. Consistent with this finding, we found no effect on earnings for men with diabetes onset in 1993–2002 (duration 1–9 years), but a significant effect for men with diabetes onset in 1983–1992 (duration ≥10 years). As regressions controlled for age, these associations were corrected for lifetime profiles in which earnings increase up to middle-age (full regression results in ESM Table 4). For women, similar negative effects on earnings were found for onset 1983–1992 and 1993–2002. Future analyses may explore potential differences in patterns related to sex.
The literature comparing employment and earnings before and after the onset of a disease is sparse. Bradley and colleagues found reduced employment among middle-aged women surviving breast cancer, but higher earnings among those who were employed [39]. On the other hand, there is a plethora of evidence on correlations between socioeconomic status and disease (ill health) using post-onset cohorts and cross-sectional design. For example, associations between the reduction in earnings and the level of functional limitation have been identified for persons with rheumatoid arthritis [40–43] and for persons with respiratory disorders [44]. For diabetes, the review by Milton and colleagues concluded, based on mostly small-sample studies, that persons with childhood onset of diabetes would experience lower employment rates and income following diabetic complications [9]. Nevertheless, correlations do not imply causation, and the role of education as a determinant of health, that is, that the effect proceeds from education to health, has been extensively analysed [45, 46]. While this direction is relevant for lifestyle-related diseases, for example, or analyses of disease management, our analysis concerns the effect of an unanticipated, significant, health-related life event and its effect on labour-market outcomes.
Earlier studies on the effect of the level of education on diabetes health outcomes have found differences regarding the time spent managing the condition and the degree of adherence to prescribed treatment [47, 48]. This paper quantifies the size of the reduction in earnings that may be attributed to diabetes onset. In a broader perspective, our findings and future analyses of the Econ-DISS data may be of relevance on a conceptual level for analyses of health and labour-market outcomes.
Finally, is the size of the earnings differential consequential? Does 5.3% lower median earnings for persons with type 1 diabetes matter? In our opinion, these differences do matter, as they correspond to the cost of 1 month’s housing for the average family after taxes. Put another way, if an employer were to pay an employee 5% less than he pays a colleague, the employee would probably want a change of employer.
The differences also suggest that further tailoring of treatment and improvement of self-management will benefit not only the individual with diabetes: society may benefit in terms of increased productivity in the labour market.
Abbreviations
- DISS:
-
Diabetes Incidence Study in Sweden
- EUR:
-
Euro
- SEK:
-
Swedish krona
References
American Diabetes Association (2008) Economic costs of diabetes in the U.S. in 2007. Diabetes Care 31:596–615
Bastida E, Pagán JA (2002) The impact of diabetes on adult employment and earnings of Mexican Americans: findings from a community based study. Health Econ 11:403–413
Brown HSI, Pagàn JA, Bastida E (2005) The impact of diabetes on employment: genetic IVs in a bivariate probit. Health Econ 14:537–544
Ingberg C, Palmer M, Aman J, Larsson S (1996) Social consequences of insulin-dependent diabetes mellitus are limited: a population-based comparison of young adult patients vs healthy controls. Diabet Med 13:729–733
Jonsson PM, Marké L-Å, Nyström L, Wall S, Östman J (2000) Excess costs of medical care 1 and 8 years after diagnosis of diabetes: estimates from young and middle-aged incidence cohorts in Sweden. Diabetes Res Clin Pract 50:35–47
Kahn ME (1998) Health and labor market performance: the case of diabetes. J Labor Econ 16:878–899
Kraut A, Walld R, Tate R, Mustard C (2001) Impact of diabetes on employment and income in Manitoba, Canada. Diabetes Care 24:64–68
Latif E (2009) The impact of diabetes on employment in Canada. Health Econ 18:577–589
Milton B, Holland P, Whitehead M (2006) The social and economic consequences of childhood-onset type 1 diabetes mellitus across the lifecourse: a systematic review. Diabet Med 23:821–829
Ng YC, Jacobs P, Johnson J (2001) Productivity losses associated with diabetes in the US. Diabetes Care 24:257–261
Tunceli K, Bradley CJ, Nerenz D, Williams LK, Pladevall M, Elston Lafata J (2005) The impact of diabetes on employment and work productivity. Diabetes Care 28:2662–2667
Vijan S, Hayward RA, Langa KM (2004) The impact of diabetes on workforce participation: results from a national household sample. Health Serv Res 39:1653–1669
Black SE, Devereux PJ, Salvanes KG (2005) Why the apple doesn’t fall far: understanding intergenerational transmission of human capital. Am Econ Rev 95:437–450
Chadwick L, Solon G (2002) Intergenerational income mobility among daughters. Am Econ Rev 92:335–345
Solon G (2002) Cross-country differences in intergenerational earnings mobility. J Econ Perspect 169:59–66
Diabetes Incidence Study in Sweden (DISS). Available from www.diss.se/index_en.htm. Accessed 18 August 2009
Östman J, Arnqvist H, Blohmé G et al (1986) Epidemiology of diabetes mellitus in Sweden. Results of the first year of a prospective study in the population age group 15–34 years. Acta Med Scand 220:437–445
Östman J, Lönnberg G, Arnqvist HJ et al (2008) Gender differences and temporal variation in the incidence of type 1 diabetes: results of 8012 cases in the nationwide Diabetes Incidence Study in Sweden 1983–2002. J Intern Med 263:386–394
WHO Expert Committee on Diabetes Mellitus (1980) Second report. World Health Organization Technical Report Series. WHO, Geneva
World Health Organization (1985) Diabetes Mellitus. Report of a WHO Study Group. Technical Report Series. WHO, Geneva
Blohmé G, Nyström L, Arnqvist H et al (1992) Male predominance in type 1 (insulin-dependent) diabetes mellitus in young adults: results of a five-year prospective nationwide study in the 15–34 year age group in Sweden. Diabetologia 35:56–62
Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (1997) Report of the Expert Committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 20:1183–1197
World Health Organization (1999) Definition, diagnosis and classification of diabetes mellitus and its complications: part 1. Diagnosis and classification of diabetes mellitus. Report of a WHO Consultation. World Health Organization, Geneva
Bakhtadze E, Borg H, Stenström G et al (2006) HLA-DQB1 genotypes, islet antibodies and beta cell function in the classification of recent-onset diabetes among young adults in the nationwide Diabetes Incidence Study in Sweden. Diabetologia 49:1785–1794
Borg H, Arnqvist H, Björk E et al (2003) Evaluation of the new ADA and WHO criteria for classification of diabetes mellitus in young adult people (15–34 yrs) in the Diabetes Incidence Study in Sweden (DISS). Diabetologia 46:173–181
Statistiska Centralbyrån [Statistics Sweden]. Available from www.scb.se/. Accessed 18 August 2009
Statistiska Centralbyrån [Statistics Sweden]. Longitudinal integration database for health insurance and labour market studies. Available from www.scb.se/Pages/List____257743.aspx. Accessed 13 August 2009
Card D (1999) The causal effect of education on earnings. In: Ashenfelter O, Card D (eds) Handbook of labor economics. Elsevier, Amsterdam, pp 1801–1863
Riksbanken [the Swedish Central Bank]. Interest and exchange rates. Annual aggregate. Available from www.riksbank.com/. Accessed 3 October 2008
Altman DG (1991) Practical statistics for medical research. Chapman & Hill, London
StataCorp (2007) Stata statistical software: release 10. Stata Corp. LP, College Station
Greene W (2000) Econometric analysis. Prentice Hall International, Upper Saddle River
Hagopian WA, Lernmark Å, Rewers MJ et al (2006) TEDDY—The Environmental Determinants of Diabetes in the Young. An observational clinical trial. Ann N Y Acad Sci 1079:320–326
Åkesson K, Nyström L, Färnkvist L, Östman J, Lernmark Å, Kockum I (2005) Increased risk of diabetes among relatives of female insulin-treated patients diagnosed at 15–34 years of age. Diabet Med 22:1551–1557
The TEDDY Study Group (2007) The Environmental Determinants of Diabetes in the Young (TEDDY) study: study design. Pediatric Diabetes 8:286–298
Blom L, Dahlquist G, Nyström L, Sandström A, Wall S (1989) The Swedish childhood diabetes study—social and perinatal determinants for diabetes in childhood. Diabetologia 32:7–13
du Prel JB, Icks A, Grabert M, Holl R, Giani G, Rosenbauer J (2007) Socioeconomic conditions and type 1 diabetes in childhood in North Rhine–Westphalia, Germany. Diabetologia 50:720–728
Eeg-Olofsson K, Cederholm J, Nilsson PM, Gudbjörnsdóttir S, Eliasson B (2007) Glycemic and risk factor control in type 1 diabetes. Diabetes Care 30:496–502
Bradley CJ, Bednarekb HL, Neumark D (2002) Breast cancer survival, work, and earnings. J Health Econ 21:757–779
Albers J, Kuper H, van Riel P et al (1999) Socio-economic consequences of rheumatoid arthritis in the first years of the disease. Rheumatology 38:423–430
Allaire S, Wolfe F, Niu J, LaValley MP, Zhang B, Reisine S (2009) Current risk factors for work disability associated with rheumatoid arthritis: recent data from a US national cohort. Arthritis Care Res 61:321–328
Burton W, Morrison A, Maclean R, Ruderman E (2006) Systematic review of studies of productivity loss due to rheumatoid arthritis. Occup Med (Lond) 56:18–27
Wolfe F, Michaud K, Choi HK, Williams R (2005) Household income and earnings losses among 6,396 persons with rheumatoid arthritis. J Rheumatol 32:1875–1883
Ward MM, Javitz HS, Smith WM, Whan MA (2002) Lost income and work limitations in persons with chronic respiratory disorders. J Clin Epidemiol 55:260–268
Bolin K, Lindgren B (2002) Asthma and allergy: the significance of chronic conditions for individual health behaviour. Allergy 57:115–122
Grossman M (2006) Education and nonmarket outcomes. In: Hanushek E, Welch F (eds) Handbook of the economics of education. Elsevier, Amsterdam, pp 577–628
Ettner SL, Cadwell BL, Russell LB et al (2009) Investing time in health: do socioeconomically disadvantaged patients spend more or less extra time on diabetes self-care? Health Econ 18:645–663
Goldman DP, Smith JP (2002) Can patient self-management help explain the SES health gradient? Proc Natl Acad Sci 99:10929–10934
Acknowledgements
We thank members of the network of diabetologists in the six healthcare regions of Sweden, who since 1983 have been responsible for data collection for DISS. The LISA database is administered by Statistics Sweden and the Social Insurance Agency, and the Swedish Agency for Innovative Systems participated in its construction. K. Steen Carlsson is indebted to the late G. Sundkvist (Lund University), former chairman of the DISS steering committee, for support in the earliest phases of compilation of the Econ-DISS database. K Steen Carlsson’s work was funded by research grants from the Foundation for Research at the Swedish Society for Diabetes (DIA 2005-005, DIA 2006-049, DIA 2007-065) and an unrestricted researcher-initiated grant from Novo Nordisk A/S, and was carried out while associated to the Vårdal Institute, the Swedish Institute for Health Sciences. DISS is supported by grants from the Swedish Research Council (2008-4026), the Juvenile Diabetes Foundation–Wallenberg Diabetes Research Program (K 98-99 JD-128 13), the Swedish Diabetes Association and the Swedish Medical Research Council (7X-14531).
Duality of interest
The authors declare that there is no duality of interest associated with this manuscript.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM Table 1
Key outcome variables from Econ-DISS from the LISA database and their original source (PDF 33 kb)
ESM Table 2
Number and percentage of cases with type 1 diabetes and controls in 1990, 1995, 2000 and 2005 by onset group (before/after) and sex (men/women) in the cohort born 1949–1970 (PDF 33 kb)
ESM Table 3
Multivariable logistic regression for the association between not being gainfully employed at least one year during 2002–2005 and diabetes duration (full results) (PDF 54.9 kb)
ESM Table 4
The effect in percentage terms on average annual earnings 2002–2005 by semi-logarithmic ordinary least squares regression (reference category in parentheses) (full regression results) (PDF 48 kb)
ESM Fig. 1
Before (a, c) and after (b, d) onset: annual employment (%) (a, b) and percentage receiving unemployment benefits (c, d) for controls (top part of each panel) and the deviation of the diabetes group (bottom part of each panel). Differences in proportion before onset (a, c) NS. After onset (b) p < 0.05 years 1993, 1995–1997, 1999–2005 and (d) p < 0.05 years 1991–1992, 1994–1996, 2001 (PDF 18.1 kb)
ESM Fig. 2
Before (a) and after (b) onset: Annual percentage having at least one period of sick leave exceeding 14 days for controls (top part of each panel) and the deviation of diabetes group (bottom part of each panel). Differences in proportion before onset (a) NS. Differences in proportion after onset (b) significant for all years (p < 0.001) (PDF 15 kb)
ESM Fig. 3
Before (a) and after (b) onset: percentage with university level of education (circles) and with compulsory level of education (7–9 years of school) (triangles). Difference between diabetes (white) and control (black) groups significant in year 1990 (proportion and χ 2; p < 0.05), otherwise, NS before onset. Difference in proportion with compulsory education significant after onset years 1993, 1997–1998, 2000–2001, 2003, 2005 (p < 0.05). Difference in proportion with university education significant after onset all years (p < 0.05). χ 2 test of independence rejected all years (p < 0.05). Difference in proportion with upper secondary level of education (not shown in figures) NS before and after onset (PDF 45.6 kb)
Rights and permissions
About this article
Cite this article
Steen Carlsson, K., Landin-Olsson, M., Nyström, L. et al. Long-term detrimental consequences of the onset of type 1 diabetes on annual earnings—evidence from annual registry data in 1990–2005. Diabetologia 53, 1084–1092 (2010). https://doi.org/10.1007/s00125-009-1625-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-009-1625-z