
Abstract
Aims/hypothesis
Increased oxidative–nitrosative stress, poly(ADP-ribose) polymerase (PARP) activation and subsequent cellular damage play important roles in the complications of both diabetes mellitus and pregnancy. Our aim was to investigate nitrative stress and PARP activity levels during normal and gestational diabetic (GDM) pregnancy in both maternal and fetal tissues.
Methods
Blood samples were collected during pregnancy (weeks 16–29 and 36–40), and placental and umbilical cord tissues were harvested after delivery from healthy volunteers and GDM patients subjected to a carbohydrate-restricted diet or insulin treatment. Immunohistochemical staining was performed on leucocytes and tissue sections using anti-nitrotyrosine (NT), anti-poly(ADP-ribose) (PAR) and anti-apoptosis inducing factor antibodies.
Results
In healthy pregnancies the intensity of NT and PAR staining of leucocytes correlated positively with gestational week (R 2 = 0.43, p < 0.01 and R 2 = 0.49, p < 0.001, respectively). In patients on a carbohydrate-restricted diet PAR staining was already strong in weeks 16–29 (p < 0.001 vs control) and did not increase further. In weeks 16–29 there was a correlation between PAR staining and the 2 h value of the oral glucose tolerance test (R 2 = 0.49, p < 0.001). Patients with the highest level of leucocyte PARP activity later required insulin therapy, which decreased the intensity of NT and PAR staining. Placental and umbilical cord tissues also had a higher level of nitrative stress markers in GDM pregnancies, but the highest level of PARP activity was observed after insulin therapy.
Conclusions/interpretation
Continuous elevation of tyrosine nitration and PARP activation may be considered physiological during pregnancy. However, the high level of PARP activity in early pregnancy may signal the subsequent development of severe GDM.
Similar content being viewed by others


Introduction
Gestational diabetes mellitus (GDM) is defined as glucose intolerance of various degrees that is first detected during pregnancy [1]. This common condition occurs in approximately 7% (range 1–14%) of all pregnancies [2]. Complications of GDM mainly affect the newborn (prematurity, macrosomia, hypoglycaemia, jaundice, respiratory distress syndrome, polycythaemia and hypocalcaemia). The maternal consequences are increased Caesarean section rate, hypertension and elevated risk of diabetes during later life [3, 4]. The number of pathological and even healthy pregnancies increases the risk of cardiovascular morbidity [5]. These clinical observations raise the possibility that GDM induces alterations in cellular metabolism in the vascular system which contribute to these complications.
It was shown previously that an increase in oxidative stress may be observed during the normal course of pregnancy [6]. High levels of oxidative stress at term deliveries may contribute to the initiation of labour or may be a result of this process [7]. GDM and pre-eclampsia are associated with a pronounced degree of oxidative stress in placental and umbilical cord tissues and also in the plasma of the mother and newborn [8–12].
Increased oxidative–nitrosative stress and consequent poly(ADP-ribose) polymerase (PARP) activation play a crucial role in the development of type 1 and type 2 diabetes and their complications [13]. Systemic hyperglycaemia triggers the generation of various reactive oxygen and nitrogen species, such as peroxynitrite, which is formed by the reaction of superoxide and nitric oxide [14, 15]. Nitration of protein tyrosine residues is one of the typical biochemical reactions induced by peroxynitrite. In addition, peroxynitrite also induces DNA single-strand breaks, which triggers the activation of the nuclear enzyme PARP. PARP uses NAD+ as a substrate to form poly(ADP-ribose) (PAR), which plays a role in numerous physiological mechanisms, such as DNA repair, regulation of genomic stability and gene expression. However, its overactivation leads to cellular dysfunction and necrotic cell death [14, 16–18]. In addition, PARP activation also leads to the translocation of apoptosis-inducing factor (AIF) from the mitochondria to the nucleus, inducing apoptotic pathways [15]. Since oxidative stress is already increased during pregnancy, its contribution to GDM-derived cardiovascular complications is difficult to determine.
The aims of the present study were: (1) to examine the degree and dynamics of oxidative–nitrosative stress and PARP activation in normal and GDM pregnancies; (2) to analyse the connection between the severity of carbohydrate intolerance and these variables; and (3) to study the effect of insulin treatment on these factors.
Methods
All procedures were approved by the ethics committee of Semmelweis University. Informed consent was signed by all participating patients.
Patients
Universal screening of GDM was done at week 16 of gestation using an OGTT with 75 g oral glucose. Those who were tested negative were retested at week 26 of gestation. Women with either fasting plasma glucose ≥7 mmol/l or 120 min post-challenge glucose ≥7.8 mmol/l were classified as having GDM according to WHO criteria [19]. Women fasted for at least 10 h before the test.
GDM patients were treated with a 160–200 g carbohydrate diet controlled by glucose self-monitoring and clinical laboratory follow-up. Insulin treatment was initiated if the fasting glucose level was >5.5 mmol/l or 1 h postprandial glucose was >7 mmol/l.
Age-matched healthy pregnant women served as controls. Women with twin pregnancy were excluded from the study. We obtained information including maternal age, height, prepregnancy weight, weight gain and medical records of deliveries. Blood samples were taken from healthy (n = 25; control group) and gestational diabetic (carbohydrate-restricted diet n = 22, insulin treatment n = 5) pregnant women during weeks 16–29 and 36–40 of pregnancy. At the same time, leucocytes were counted, C-reactive protein was measured and liver and kidney function was tested. In the second phase of the study we collected placenta and umbilical cord tissues from similar groups of patients (control n = 6, carbohydrate-restricted diet n = 9, insulin treatment n = 5) after delivery.
Immunohistochemistry
Leucocytes were isolated from blood samples using Histopaque-1077 (Sigma Aldrich, St Louis, MO, USA). Methanol-fixed smears were prepared from the cell suspension. Anti-nitrotyrosine rabbit polyclonal antibody (Upstate Biotechnology, Lake Placid, NY, USA) (1:80, 4°C, overnight) was used to stain 3-nitrotyrosine, the marker of tyrosine nitration. Poly(ADP-ribose) was detected using a mouse monoclonal anti-PAR antibody (Calbiochem, San Diego, CA, USA) (1:1,000, 4°C, overnight) after antigen retrieval (0.1 mmol/l citrate buffer, pH 3, heated in a microwave oven for 15 min).
Secondary labelling was achieved using biotinylated anti-mouse horse or anti-rabbit goat antibodies (Vector Laboratories, Burlingame, CA, USA) (30 min, room temperature). Horseradish peroxidase-conjugated avidin (30 min, room temperature) and nickel-enhanced diaminobenzidine (6 min, room temperature, black colour) was used to visualise the labelling (Vector Laboratories). Smears were counterstained with nuclear fast red.
To determine the proportion of NT-positive cells, at least 300 cells were counted in each slide and the percentage of all positively stained cells was recorded by a blinded observer. To evaluate PAR-stained slides, a semiquantitative PAR-positivity score was determined by a blinded observer (1, no staining; 2, light cytoplasmic staining; 3, strong cytoplasmic staining; 4, cytoplasmic staining with a few positive nuclei; 5, approximately 50% of the nuclei positive; 6, approximately 75% of the nuclei positive; 7, general nuclear staining with a few negative cells; 8, all nuclei positive; 9, strong nuclear staining in all cells; 10, very strong general nuclear staining in all cells [20]).
Samples of placenta and umbilical cord were embedded in paraffin then fixed with formalin. After deparaffinisation and antigen retrieval (0.1 mol/l citrate buffer, pH 3/pH 6, heated in microwave oven for 15 min), sections were incubated overnight at 4°C with primary antibodies: polyclonal anti-PAR (Calbiochem) at a dilution of 1:3,200, polyclonal anti-nitrotyrosine (Upstate) at a dilution of 1:200 and rabbit anti-AIF polyclonal antibody (Chemicon International, Temecula, CA, USA) at a dilution of 1:100. Biotinylated anti-rabbit goat antibody (Vector Laboratories) was used as secondary antibody for 30 min at room temperature. Horseradish peroxidase-conjugated avidin (Vector Elite Kit; Vector Laboratories) was applied for 30 min at room temperature. Diaminobenzidine (Vector Laboratories) was used to visualise labelling. The sections were counterstained with haematoxylin. Positivity of specific staining was determined by a blinded experimenter on a scale of 1–10.
Statistical analysis
Results are expressed as mean ± SEM. Analysis of variance with Tukey’s post hoc test was used to compare mean values. Linear regression was used to analyse correlation between variables.
Results
Patient characteristics
Clinical data of the three groups of patients are summarised in Table 1 (leucocytes) and Table 2 (placenta and umbilical cord). No significant differences were found in demographic variables (age, height, weight, BMI and numbers of pregnancies and deliveries). Leucocyte count, C-reactive protein, liver and kidney function were all in the physiological range. Weight gain during pregnancy was lower in gestational diabetic pregnancies but it reached statistical significance only in the first phase of the experiment. The 2 h value of the diagnostic OGTT was significantly higher in GDM patients compared with controls (this was the diagnostic criterion). The long-term indicators of carbohydrate metabolism, such as fructosamine (160 ± 10 μmol/l, normal value <285 μmol/l) and HbA1c (5.7 ± 0.3%, normal range 4.4–6.4%), were in the normal range in all groups of patients. The 1 h postprandial glucose level at the time of leucocyte sampling was similar in the two GDM groups. However, significantly higher average glucose values (mean of multiple tests during treatment) were found in the insulin-treated group of patients whose placentas were examined compared with patients subjected to carbohydrate-restricted diet. The higher postprandial glucose value was the indication of starting or increasing the dose of insulin treatment. No significant differences were found in the time, mode of delivery or neonatal anthropometrical data.
Immunostaining
Leucocytes
Tyrosine nitration was significantly increased during weeks 36–40 of pregnancy compared with weeks 16–29 in both the healthy and carbohydrate-restricted diet GDM groups. On the other hand, insulin treatment significantly decreased the nitrotyrosine staining for the last 4 weeks of pregnancy (Fig. 1).

Immunostaining of leucocyte smears. a Percentage of NT-positive cells in the three groups of patients in gestational weeks 16–29 and 36–40. b PAR score of leucocyte smears. Data are mean and SEM. White columns, control group; black columns, carbohydrate-restricted diet; grey columns, insulin treatment. *p < 0.05, **p < 0.01 ***p < 0.001 c Representative images of smears stained with NT antibody. Arrows show positive cells (black). Nuclear fast red counterstaining appears in red. d Representative images of smears stained for PAR. Positive cells appear in different tones of grey depending on staining strength. Nuclear fast red was used as counterstain
Similarly, the PAR content of circulating leucocytes was significantly higher in the carbohydrate-restricted diet group compared with the control group in weeks 16–29. This difference was abolished by weeks 36–40 of pregnancy. Whereas PARP activity increased constantly during the course of pregnancy in healthy pregnant women, in GDM patients subjected to the carbohydrate-restricted diet high PARP activity was already observed at the time of diagnosis and activity did not increase further after the 29th week. However, insulin treatment significantly reduced PARP activity by weeks 36–40 (Fig. 1). Linear regression analysis confirmed the correlation between time and the degree of nitrative stress and PARP activity in healthy patients (Fig. 2).

Correlations of gestational week and OGTT 2 h results with NT staining and PARP activity of leucocytes. a Effect of gestational week on the number of NT-positive cells. Slope 1.22 ± 0.35, R 2 = 0.43, p < 0.01. b Effect of gestational week on the PAR score of leucocyte smears. Slope 0.12 ± 0.01, R 2 = 0.49, p < 0.001. c Relationship between OGTT 2 h results (mmol/l) and the number of NT-positive leucocytes. No correlation was found. d Relationship between OGTT 2 h results (mmol/l) and PAR activity of leucocytes. Slope 0.63 ± 0.14, R 2 = 0.49, p < 0.001. Arrows show data for patients subjected to the carbohydrate-restricted diet who later required insulin. Black diamonds, control group; black circles, patients in gestational weeks 16–29; white triangles, insulin-treated patients in gestational weeks 36–40
Comparing the results of the 120 min value from the OGTT with the PARP activity revealed a linear correlation in weeks 16–29 but not weeks 36–40. Further analysis of participants in the carbohydrate-restricted diet group showed that those who later required insulin treatment had the highest PARP activity earlier. The effect of insulin treatment with respect to reduction of PARP activity was most apparent when we compared this group with the insulin-treated group in weeks 36–40 (Fig. 2). However, results for the insulin-treated patients in weeks 36–40 indicate that in these patients PAR staining was similar to that in the other two groups, but lower than values at weeks 16–29 in patients subjected to carbohydrate-restricted diet who later needed insulin treatment (Fig. 2).
Placenta and umbilical cord
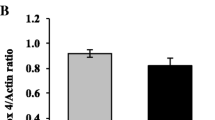
Tyrosine nitration in the placenta and umbilical artery was significantly greater in insulin-treated GDM patients compared with control and GDM patients subjected to the carbohydrate-restricted diet. In the umbilical veins we found a difference only between the insulin-treated and the control group (Figs 3 and 4a). In all tissues examined, PARP activity was significantly higher in the insulin-treated group compared with the group on the carbohydrate-restricted diet. There was also a significant difference between insulin-treated and control participants in placental tissues (Figs 3 and 4b). AIF translocation showed a significant difference only in placental tissue between the insulin-treated and the control groups (Figs 3 and 4c).

Results of immunostaining of placental and umbilical cord tissues. a Intensity of NT staining in the three groups. b PARP activity (intensity of PAR staining) in the three groups. c Intensity of AIF staining in the three groups Data are mean and SEM. White columns, control group; black columns, carbohydrate-restricted diet; grey column, insulin treatment. *p < 0.05, **p < 0.01 ***p < 0.001

Representative immunohistochemical images. a Representative images of tissues stained with NT antibody. Positive staining appears in different tones of brown depending on staining strength. Haematoxylin (blue) was used as counterstain. b Representative images of tissues stained against PAR. c Representative images of tissues stained for AIF
Discussion
There are only a few studies about the association between maternal oxidative stress and normal pregnancy. It has been shown that oxidative stress increases during the course of pregnancy [6, 7, 21, 22]. Toescu and colleagues [6] found that plasma hydroperoxides increases from trimester to trimester. However, they measured this variable only at the 12th, 24th and 36th weeks, so they could not determine the dynamics of this phenomenon. According to our data there is a continuous elevation of nitrative stress and PARP activity in maternal circulating leucocytes from the 16th week, with a linear correlation between gestational week and these variables. These results may suggest that the continuous elevation of nitrative stress and PARP activation is a physiological phenomenon of human pregnancy.
Recent studies have raised the possibility that protein nitration by peroxynitrite is not only a pathological event but is also a post-translational modification with regulatory roles which may be beneficial during pregnancy. Peroxynitrite and subsequent protein nitration may induce vasodilatation, muscle relaxation, depression of the proliferative response of activated T cells, and attenuated platelet activation [23–26]. On the other hand the phrase ‘physiological phenomenon’ does not necessary imply any advantage; for example, ageing is also associated with increased oxidative–nitrosative stress and PARP activation [27]. Various studies have examined the connections of parity with cardiovascular morbidity and mortality and have found that multiparous women have an increased risk of developing coronary heart disease and other cardiovascular diseases. In their recent paper, Tawfik et al. [28] suggested that the increased oxidative stress and peroxynitrite formation during pregnancy play important roles in this phenomenon. They found reduced endothelium-dependent relaxation in the coronary arteries and aortic rings of multiparous rats, which was associated with increased oxidative stress and could be prevented by the peroxynitrite scavenger FeTPPs (5,10,15,20-tetrakis(4-sulfonatophenyl)porphyrinato iron (III) chloride).
On the other hand, our results showed that in GDM pregnancies the PARP activity of leucocytes was already elevated in the middle of pregnancy and did not increase subsequently. The analysis of the severity of carbohydrate intolerance (the 2 h OGTT value) and PARP activity of circulating leucocytes revealed a linear correlation between these factors. We also found that those patients whose leucocytes had the highest PAR score in the middle of pregnancy later required insulin treatment. Subsequently, insulin treatment decreased both nitrative stress and PARP activity in these cells, signalling a casual relationship between high glucose levels and PARP activity.
The early elevation of PARP activation in GDM patients may contribute to the development of various complications of pregnancy. It has been shown that oxidative stress increases at the onset of labour regardless of its dating [7, 21, 22]. The higher rate of preterm deliveries in these patients may be related to the early PARP activation. The common characteristic of pre-eclampsia and late vascular complications of diabetes is endothelial dysfunction, in which oxidative–nitrosative stress and PARP activation play key pathogenic roles [12, 16]. The early increase in PARP activity may explain the higher prevalence of pre-eclampsia among GDM pregnancies.
Because the elevation of PARP activity occurs earlier in GDM patients, they spend a longer time in this state than healthy pregnant women, which may give a potential explanation for their increased risk of complications after pregnancy. PARP activation also plays a role in the pathogenesis of type 1 and type 2 diabetes. It is involved in the autoimmune destruction of pancreatic beta cells [29]. Increased PARP activity can be measured in skin biopsies not only in patients with type 2 diabetes but also in healthy people with a parental history of type 2 diabetes (i.e. those with a higher risk of developing the disease) [30]. The prolonged PARP activation in GDM patients may be involved in the development of carbohydrate intolerance in later life or in the development of late cardiovascular complications. This hypothesis is consistent with the fact that cardiovascular risk also increases with the number of healthy pregnancies, which is related to increased oxidative–nitrosative stress during pregnancy [5, 28].
The linear association between the 2 h OGTT value and the PARP activity of circulating leucocytes suggests that not only GDM patients but also women with OGTT values below the diagnostic criterion might be at increased risk. This hypothesis is concordant with the observation of the Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) study, which showed a continuous association between maternal glucose level and adverse pregnancy outcome [31].
The nitrative stress and PARP activation in placental and umbilical cord vessels did not differ between patients subjected to the carbohydrate-restricted diet and control patients, a result similar to that for leucocytes from the last weeks of pregnancy. While insulin treatment decreased these variables in circulating leucocytes of the mother, in placental tissues of the fetal side we detected increased NT, PAR and AIF translocation.
A limitation of our study is that it included only five insulin-treated GDM patients, and, for ethical reasons, no patient had similar carbohydrate metabolism as insulin-treated GDM patents without insulin treatment. As a consequence, we were unable to detect the possible positive effects of insulin treatment in the placental and umbilical cord tissues. In addition, according to our data there seems to be maximal PARP activation in circulating leucocytes, so we cannot exclude the possibility that leucocytes with higher PARP activation die and are eliminated from the circulation.
On the other hand, in the insulin-treated severe GDM group the excess hyperglycaemia and consequent oxidative–nitrosative stress might have induced definitive pathological events, such as nitration of critical signalling molecules [32]. Irreversible alterations of these proteins may lead to compromised placental function, which cannot be attenuated by insulin treatment. Our present results indicate that nitrative stress affects the vascular elements of the placenta, an observation that is supported by studies from the group of Myatt, who showed nitration of endothelial nitric oxide synthase, cyclooxygenase and prostacyclin synthase [32–34]. These alterations in the main vasoactive enzyme systems in the vascular wall lead to endothelial dysfunction, which may trigger vasoconstriction, platelet aggregation and apoptosis [32].
There are also some major differences between the cell types we examined that may explain our results. First, while there are not only insulin-insensitive (GLUT1, GLUT3) but also insulin-sensitive (GLUT4) glucose transporters on leucocytes [35], glucose transport through the placenta is known to be insulin-independent facilitated diffusion, basically through the action of GLUT1. Contrary to trophoblast cells, in which insulin elevates the amount of GLUT1 on the basal membrane, in circulating leucocyte it fails to alter GLUT1 production [35, 36]. As a result of insulin treatment, the level of GLUT4 increases in leucocytes, reducing insulin resistance [35]. In our previous experiments we had already observed that the effect of insulin treatment on PARP activity was different between circulating leucocytes and vascular endothelial cells. In type 1 diabetic rats, an oscillating blood glucose level induced by insulin treatment (a model of poor glycaemic control) resulted in an increase in PARP activity in vascular endothelial cells but not in circulating leucocytes compared with animals whose blood glucose level was completely normalised by insulin (a model of good glycaemic control) [37]. Additionally, we have previously shown in vitro that under high-glucose conditions insulin reduces the PARP activity of circulating leucocytes to a small extent (5%), independently of its glucose-lowering effect [38]. However, this does not seem to be an adequate explanation of the significantly decreased PARP activity observed in GDM patients in the present study, so it may be assumed that the combined effect of insulin, both directly on the leucocytes and indirectly by lowering glucose levels, is responsible for the reduction of PARP activity under insulin treatment.
According to our data, the PARP activity of circulating leucocytes of pregnant women is influenced by the gestational week, the severity of carbohydrate intolerance and the treatment modality. On the other hand, in placental and umbilical cord tissues PARP activity is mainly affected by the severity of carbohydrate intolerance (Fig. 5) The observation that the insulin requirement was predicted by the high PARP activity of circulating leucocytes suggests that measuring this variable might be used as an early predictive marker to identify patients with a high risk of developing severe GDM.

Hypothetic dynamics of PARP activity in circulating leucocytes during pregnancy and in placental/umbilical cord tissues after delivery. The thickness of the grey shapes represents the degree of PARP activity. The PARP activity of circulating leucocytes increases with advancing gestational week and also with the severity of carbohydrate intolerance, represented by the 2 h OGTT value. The highest PARP activity was measured in patients who later required insulin treatment; however, receiving insulin decreased PARP activity. Because of ethical concerns, we were unable to examine severe GDM patients without insulin treatment. On the other hand, in placental and umbilical cord tissues PARP activity increased only in severe GDM, which suggests that it is mainly affected by the severity of carbohydrate intolerance
Abbreviations
- GDM:
-
Gestational diabetes mellitus
- PAR:
-
Poly(ADP-ribose)
- PARP:
-
Poly(ADP-ribose) polymerase
- AIF:
-
Apoptosis inducing factor
References
Buchanan TA, Xiang AH (2005) Gestational diabetes mellitus. J Clin Invest 115:485–491
Setji TL, Brown AJ, Feinglos MN (2005) Gestational diabetes mellitus. Clin Diab 23:17–24
Kjos SL, Buchanan TA (1999) Gestational diabetes mellitus. N Engl J Med 341:1749–1756
Kim C, Newton KM, Knopp RH (2002) Gestational diabetes and the incidence of type 2 diabetes: a systematic review. Diabetes Care 25:1862–1868
Humphries KH, Westendorp IC, Bots ML et al (2001) Parity and carotid artery atherosclerosis in elderly women: the Rotterdam Study. Stroke 32:2259–2264
Toescu V, Nuttall SL, Martin U et al (2004) Changes in plasma lipids and markers of oxidative stress in normal pregnancy and pregnancies complicated by diabetes. Clin Sci (Lond) 106:93–98
Fainaru O, Almog B, Pinchuk I, Kupferminc MJ, Lichtenberg D, Many A (2002) Active labour is associated with increased oxidisibility of serum lipids ex vivo. BJOG 109:938–941
Myatt L, Cui X (2004) Oxidative stress in the placenta. Histochem Cell Biol 122:369–382
Coughlan MT, Vervaart PP, Permezel M, Georgiou HM, Rice GE (2004) Altered placental oxidative stress status in gestational diabetes mellitus. Placenta 25:78–84
Raijmakers MT, Dechend R, Poston L (2004) Oxidative stress and preeclampsia: rationale for antioxidant clinical trials. Hypertension 44:374–380
Raijmakers MT, Roes EM, Poston L, Steegers EA, Peters WH (2008) The transient increase of oxidative stress during normal pregnancy is higher and persists after delivery in women with pre-eclampsia. Eur J Obstet Gynecol Reprod Biol 138:39–44
Sankaralingam S, Xu Y, Sawamura T, Davidge ST (2009) Increased lectin-like oxidized low-density lipoprotein receptor-1 expression in the maternal vasculature of women with preeclampsia: role for peroxynitrite. Hypertension 53:270–277
Szabo C (2009) Role of nitrosative stress in the pathogenesis of diabetic vascular dysfunction. Br J Pharmacol 156:713–727
Pacher P, Liaudet L, Soriano FG, Mabley JG, Szabo E, Szabo C (2002) The role of poly(ADP-ribose) polymerase activation in the development of myocardial and endothelial dysfunction in diabetes. Diabetes 51:514–521
Obrosova IG, Mabley JG, Zsengeller Z et al (2005) Role for nitrosative stress in diabetic neuropathy: evidence from studies with a peroxynitrite decomposition catalyst. FASEB J 19:401–403
Soriano FG, Virag L, Szabo C (2001) Diabetic endothelial dysfunction: role of reactive oxygen and nitrogen species production and poly(ADP-ribose) polymerase activation. J Mol Med 79:437–448
Brownlee M (2001) Biochemistry and molecular cell biology of diabetic complications. Nature 414:813–820
Virag L, Szabo C (2002) The therapeutic potential of poly(ADP-ribose) polymerase inhibitors. Pharmacol Rev 54:375–429
World Health Organization (1999) Definition, diagnosis, and classification of diabetes mellitus and its complications: report of a WHO consultation. Available from http://whqlibdoc.who.int/hq/1999/WHO_NCD_NCS_99.2.pdf, accessed 10 June 2009
Toth-Zsamboki E, Horvath E, Vargova K et al (2006) Activation of poly(ADP-ribose) polymerase by myocardial ischemia and coronary reperfusion in human circulating leukocytes. Mol Med 12:221–228
Nakai A, Oya A, Kobe H et al (2000) Changes in maternal lipid peroxidation levels and antioxidant enzymatic activities before and after delivery. J Nippon Med Sch 67:434–439
Yaacobi N, Ohel G, Hochman A (1999) Reactive oxygen species in the process of labor. Arch Gynecol Obstet 263:23–24
Brito C, Naviliat M, Tiscornia AC et al (1999) Peroxynitrite inhibits T lymphocyte activation and proliferation by promoting impairment of tyrosine phosphorylation and peroxynitrite-driven apoptotic death. J Immunol 162:3356–3366
Low SY, Sabetkar M, Bruckdorfer KR, Naseem KM (2002) The role of protein nitration in the inhibition of platelet activation by peroxynitrite. FEBS Lett 511:59–64
Mondoro TH, Shafer BC, Vostal JG (1997) Peroxynitrite-induced tyrosine nitration and phosphorylation in human platelets. Free Radic Biol Med 22:1055–1063
Ferdinandy P (2006) Peroxynitrite: just an oxidative/nitrosative stressor or a physiological regulator as well? Br J Pharmacol 148:1–3
Pacher P, Beckman JS, Liaudet L (2007) Nitric oxide and peroxynitrite in health and disease. Physiol Rev 87:315–424
Tawfik HE, Cena J, Schulz R, Kaufman S (2008) Role of oxidative stress in multiparity-induced endothelial dysfunction. Am J Physiol Heart Circ Physiol 295:H1736–H1742
Burkart V, Wang ZQ, Radons J et al (1999) Mice lacking the poly(ADP-ribose) polymerase gene are resistant to pancreatic beta-cell destruction and diabetes development induced by streptozocin. Nat Med 5:314–319
Szabo C, Zanchi A, Komjati K et al (2002) Poly(ADP-Ribose) polymerase is activated in subjects at risk of developing type 2 diabetes and is associated with impaired vascular reactivity. Circulation 106:2680–2686
HAPO Study Cooperative Research Group, Metzger BE, Lowe LP et al (2008) Hyperglycemia and adverse pregnancy outcomes. N Engl J Med 358:1991–2002
Webster RP, Roberts VH, Myatt L (2008) Protein nitration in placenta—functional significance. Placenta 29:985–994
Stanek J, Eis AL, Myatt L (2001) Nitrotyrosine immunostaining correlates with increased extracellular matrix: evidence of postplacental hypoxia. Placenta 22(Suppl A):S56–S62
Roberts VH, Smith J, McLea SA, Heizer AB, Richardson JL, Myatt L (2009) Effect of increasing maternal body mass index on oxidative and nitrative stress in the human placenta. Placenta 30:169–175
Calder PC, Dimitriadis G, Newsholme P (2007) Glucose metabolism in lymphoid and inflammatory cells and tissues. Curr Opin Clin Nutr Metab Care 10:531–540
Illsley NP (2000) Glucose transporters in the human placenta. Placenta 21:14–22
Horvath EM, Benko R, Kiss L et al (2009) Rapid ‘glycaemic swings’ induce nitrosative stress, activate poly(ADP-ribose) polymerase and impair endothelial function in a rat model of diabetes mellitus. Diabetologia 52:952–961
Horvath EM, Benko R, Gero D, Kiss L, Szabo C (2008) Treatment with insulin inhibits poly(ADP-ribose)polymerase activation in a rat model of endotoxemia. Life Sci 82:205–209
Acknowledgements
This work was supported by the National Institutes of Health (NIH R01 GM060915), the Hungarian Scientific Research Fund, Budapest, Hungary (OTKA; D45933, T049621), TÉT A4/04, TÁMOP 4.2.2-08/1/KMR-2008-0004, Bolyai and Öveges Fellowships and the Zsigmond Diabetes Foundation (Budapest, Hungary).
Duality of interest
C. Szabo is a stockholder of Inotek Pharmaceuticals (Lexington, MA, USA), a company involved in the development of poly(ADP-ribose) polymerase (PARP) inhibitors and antioxidants. Other authors declare no duality of interest associated with this manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
E. M. Horváth and R. Magenheim contributed equally to this study.
Rights and permissions
About this article
Cite this article
Horváth, E.M., Magenheim, R., Kugler, E. et al. Nitrative stress and poly(ADP-ribose) polymerase activation in healthy and gestational diabetic pregnancies. Diabetologia 52, 1935–1943 (2009). https://doi.org/10.1007/s00125-009-1435-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-009-1435-3