
Abstract
Aims/hypothesis
We investigated relations between fasting blood glucose and the incidence of cancer.
Methods
A population-based cohort of more than 140,000 Austrian adults (63,585 men, 77,228 women) was followed over an average of 8.4 years. Incident cancer (other than non-melanoma skin cancers) was ascertained by a population-based cancer registry (n=5,212). Cox proportional-hazards models were used to estimate hazard rate ratios (HR) stratified for age and adjusted for smoking, occupational group and body mass index.
Results
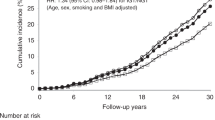
The highest fasting blood glucose category (≥7.0 mmol/l) was weakly associated with all cancers combined (HR 1.20; 95% CI, 1.03–1.39 in men and 1.28; 95% CI, 1.08–1.53 in women) relative to the reference level (4.2–5.2 mmol/l). The strongest association was found for liver cancer in men (HR 4.58; 95% CI, 1.81–11.62). Positive associations between fasting hyperglycaemia (6.1–6.9 or ≥7.0 mmol/l) and cancer incidence were also observed for non-Hodgkin’s lymphoma in men, and for colorectal and bladder cancer in women. Breast cancer in women diagnosed at or after age 65 was also associated with fasting blood glucose ≥7.0 mmol/l. Positive associations with glucose values >5.3 mmol/l were noted for thyroid cancer, gallbladder/bile duct cancer and multiple myeloma in men and women combined.
Conclusions/interpretation
These findings provide further evidence that elevated blood glucose is associated with the incidence of several types of cancer in men and women.
Similar content being viewed by others


Introduction
Many studies have examined the relation between diabetes mellitus and individual cancers. Associations with liver and pancreatic cancers, and to a somewhat lesser extent with colon and endometrial cancers, are well established [1–9]. The inconsistent findings of studies investigating elevated blood glucose levels and other cancers [10–16] may be the result, at least in part, of the use of different endpoints (cancer mortality vs incidence), exposure criteria (fasting glucose vs glucose tolerance tests) and small sample sizes. Three studies have examined associations between abnormal glucose tolerance and mortality due to different specific cancer types in a single population [17–19]. To our knowledge, the relation between fasting blood glucose and incident cancers ascertained by a population-based cancer registry has been investigated in one Icelandic [20] and one large Korean [21] study cohort only. We conducted a prospective investigation of associations between baseline fasting blood glucose values and the incidence of specific cancers and of all cancers combined (excluding non-melanoma skin cancers) in a population-based cohort of more than 140,000 Austrian men and women followed for an average of >8 years.
Subjects, materials and methods
Study population
The Vorarlberg Health Monitoring and Promotion Programme (VHM&PP) is carried out in Vorarlberg, the westernmost province of Austria. It is routinely performed by the Agency of Social and Preventive Medicine and is offered annually to all Vorarlberg residents over 19 years of age. The screening examination takes place in the practices and includes a physical examination, a blood test and a consultation with a doctor. Enrolment is voluntary and costs are covered by the participant’s (compulsory) health insurance. The screening programme is well-publicised and widely accepted, and more than two-thirds of Vorarlberg residents aged 35–54 years have participated in at least one examination since the programme began in 1985 [22].
Between 1988 and 2001, 155,820 adult Vorarlberg residents were enrolled in the VHM&PP Study Cohort after signing an informed consent to store and process personal data and biological samples. The current analysis was restricted to participants with complete data on blood glucose, height, weight and occupational group at baseline. Participants were also excluded if they had <1 year of follow-up (n=6,048), or were diagnosed with cancer (other than non-melanoma skin cancer) before or within 1 year following enrolment (n=2,121). Data pertaining to the first year of follow-up were not included in analyses.
Blood glucose
A blood glucometer calibrated to plasma venous glucose was used to determine fasting morning glucose levels from capillary-derived samples. Glucose values were divided into quartiles based on the distribution among all study participants. The upper quartile (≥5.3 mmol/l) was subdivided into three additional categories using 2002 WHO clinical threshold values for impaired fasting glycaemia (6.1–6.9 mmol/l) and diabetes (≥7.0 mmol/l) [23]. (Blood glucose values in mmol/l correspond to mg/dl×0.0555.) Participants with glucose values in the second and third quartiles (4.2–5.2 mmol/l) were the reference group for all comparisons. This approach made it possible to investigate—in addition to risks associated with hyperglycaemic levels—the risks associated with glucose levels in the lower (2.2–4.1 mmol/l) and upper (5.3–6.0 mmol/l) normoglycaemic ranges. Information about pre-existing type 1 or type 2 diabetes was not available.
Outcomes
Incident cancers were identified by the Vorarlberg cancer registry, which has been accepted for IARC publication since 1993 [24]. The proportion of cancers discovered by death certificate only (DCO) is an indicator of the completeness of cancer registry ascertainment, with DCO rates of 5–10% expected for registries in developed countries. The 1993–1997 Vorarlberg cancer registry DCO rate was 7% for men and 9% for women [25] and 5% for both sexes in 1998–2002 (personal communication, W. Oberaigner, Cancer Registry of Tyrol). Nearly all cancers were histologically verified and coded according to the ninth revision of the International Classification of Diseases (ICD-9). Cohort data were linked with the Vorarlberg Death Index to identify deaths and to calculate person-years at risk.
Covariates
Participants were classified as current, former or never smokers. Participants who never smoked could not be distinguished from those who did not respond to questions about smoking at baseline, but baseline smoking status was verified for more than 70% of study participants based on information provided at subsequent examinations. Occupational group (blue collar, white collar or self-employed) was determined from each participant’s insurance number, and was included in models as a surrogate measure of socioeconomic status. Participants who were retired at baseline were classified according to their former occupation, and housewives were classified according to their husband’s job. BMI was determined from baseline height and weight measurements and categorised based on clinical guidelines (<25 kg/m2; 25 to <30 kg/m2; ≥30.0 kg/m2) [26].
Statistical analysis
Cox proportional-hazards models were used to compute hazard rate ratios (HR) and 95% confidence intervals (95% CI) for the index fasting glucose categories relative to the reference group (4.2–5.2 mmol/l). Cox models were stratified according to age at baseline by including age (in years) in the strata statement, and were adjusted for smoking, occupational group and BMI. Linear trends were tested by modelling an ordinal variable indicating the median value of each participant’s glucose category, with Wald p values <0.05 considered statistically significant. All calculations were carried out with SAS version 8.2 software.
Associations specific to the subject’s sex were estimated for all cancers combined (excluding non-melanoma skin cancers) and for specific cancers with at least 40 cases in either of the sexes. Associations with less common cancers were estimated for men and women combined if there were at least five cases in each exposure category; hyperglycaemic categories (6.1–6.9 and ≥7 mmol/l) were combined as necessary. Associations between blood glucose and breast cancer were estimated for all women and according to age at diagnosis (<50, 50 to<65, and ≥65 years and older), because the association between overweight and breast cancer has been shown to differ with menopausal status and may differ by age among postmenopausal women [27, 28]. Person-years at risk for age-specific models were assigned to the age interval in which they were accumulated.
Results
The final study cohort consisted of 63,585 men and 77,228 women with a mean age at baseline of 43 years (Table 1). The average length of follow-up was 8.4 years (range 1–14), and the total time at risk exceeded 1.1 million person-years. Average fasting blood glucose values were 4.9 and 4.8 mmol/l for men and women, respectively (range 2.2–26.6 mmol/l). Over 5,000 cancers were diagnosed, with an average age at diagnosis of 64 years (range 22–96).
There was a weak positive association between elevated glucose values (>6.1 mmol/l) and the incidence of all cancers combined in both men and women (Tables 2 and 3). The strongest positive association was observed for liver cancer in men (Table 2), which was increased in association with high normal as well as hyperglycaemic glucose levels. Effect estimates for men and women combined were consistent with those for men only (Table 4). Non-Hodgkin’s lymphoma was positively associated with blood glucose values above the reference range in men, although the association was somewhat stronger for blood glucose 6.1–6.9 mmol/l than for ≥7.0 mmol/l (Table 2), and there was no association with non-Hodgkin’s lymphoma in women. There was a weak positive association between colorectal cancer and fasting blood glucose values between 6.1 and 6.9 mmol/l among both men (HR 1.37; 95% CI, 0.94–2.01) and women (HR 1.57; 95% CI, 1.08–2.28), but blood glucose ≥7.0 mmol/l was not clearly associated with risk. Combined estimates for men and women also indicated positive associations in both the high normal (5.3–6.0 mmol/l) and the hyperglycaemic ranges with liver cancer, thyroid cancer, multiple myeloma, and with gallbladder and bile duct cancer (Table 4). The association between fasting blood glucose ≥7.0 mmol/l and breast cancer in women (HR 1.38; 95% CI, 1.02–1.86) appeared to be driven by cases of breast cancer diagnosed among women aged ≥65 years (HR 1.62; 95% CI, 1.12–2.34), which accounted for 37 of the 50 breast cancer cases associated with this level of fasting glucose (Table 5).
Several cancers that were associated with elevated glucose levels were also positively associated with low fasting blood glucose levels (2.2–4.1 mmol/l), including bladder and thyroid cancers in women, non-Hodgkin’s lymphomas, liver and pancreatic cancers in men, and multiple myelomas in men and women combined; however, estimates were not statistically significant. Low blood glucose levels were inversely associated with kidney cancer in men and pancreatic cancer in women.
Discussion
Several studies have reported elevated risks for specific cancers among diabetic compared with non-diabetic patients, but only a few have prospectively evaluated associations between incident cancers and fasting glucose levels within the normal range [10, 12, 21]. We evaluated blood glucose over the complete glucose distribution and found that glucose values consistent with impaired fasting glycaemia and diabetes were associated with all cancers combined in both men and women. However, estimated risks of several cancers were also increased in association with high normal fasting blood glucose values and with low glucose values relative to the reference range.
Biological mechanisms that might link elevated blood glucose values to carcinogenesis are poorly understood. In late-stage type 2 diabetes mellitus, malfunction of pancreatic beta cells leads to an absolute insulin deficiency; however, the onset of type 2 diabetes mellitus is usually preceded by a long asymptomatic phase characterised by insulin resistance and hyperinsulinaemia. Growth-promoting effects of insulin and insulin-like growth factor [29, 30] have been proposed as a causal link between abnormal glucose metabolism and colon, breast and prostate cancers [31]. Elevated BMI has been associated with several types of cancer [31] and was positively correlated with blood glucose in this study cohort (r=0.21); however, the associations observed appeared to be independent of baseline BMI.
Liver cancer in men was strongly associated with elevated fasting blood glucose in our study population. This finding was based on only 45 cases in men and 16 cases in women but was consistent with previous studies of incident liver cancer and elevated fasting glucose [21] or diabetes [1, 9, 32]. Diabetes is associated with fatty liver disease and cirrhosis, which are also risk factors for liver cancer [33]. Alcohol consumption might confound the association between elevated blood glucose levels and liver cancer but we were unable to control for this in our analyses.
We noted a positive association between elevated fasting blood glucose and non-Hodgkin’s lymphoma in men. Although small studies have reported associations between diabetes and non-Hodgkin’s lymphoma [34, 35], two prospective studies found no association with hospitalisation for diabetes [1, 2], and a combined series of case-control studies in northern Italy reported an inverse association between diabetes mellitus and incident non-Hodgkin’s lymphoma [3].
There are conflicting data concerning associations between diabetes and breast cancer [1, 3, 4, 11, 12, 21]. We noted a weak association with fasting glucose ≥7.0 mmol/l only, which appeared to be specific to women diagnosed with breast cancer at age 65 or older. This resulted in a weaker association between glucose and breast cancer among women as a whole, which may explain the inconsistent findings in studies that estimated associations for women without regard to age or menopausal status.
We observed a positive association between fasting glucose ≥6.1 mmol/l and bladder cancer in women only, based on 11 exposed cases. Hyperglycaemia may increase urinary tract infections, and a positive relationship between cystitis and bladder cancer has been reported [36, 37].
Few studies have included sufficient numbers of cases to evaluate associations between diabetes and gallbladder/bile duct cancer, thyroid cancer or multiple myeloma. We observed strong positive associations with fasting glucose levels ≥5.3 mmol/l for all three of these cancers in men and women combined; however, estimates were based on small numbers of cases. Diabetes is a risk factor for gallstones, and gallstones are an established risk factor for gallbladder cancer. Positive associations between elevated glucose levels and gallbladder carcinoma and multiple myeloma are consistent with findings from a Danish record linkage study of incident cancers and hospitalisation for diabetes [1]. To our knowledge, positive associations between high-normal or hyperglycaemic fasting glucose values and thyroid cancer have not been described previously.
Major strengths of the study are its prospective design and the large number of study participants. The incident cancers were ascertained by an established population-based cancer registry and nearly all the cases were histologically confirmed; therefore, the likelihood of outcome misclassification was low. Our use of a single fasting blood glucose measurement as a proxy measure of abnormal glucose metabolism may have resulted in some non-differential misclassification because we could not account for the variations caused by day to day fluctuations in individual blood glucose levels. Variability in laboratory methods also may have influenced results because blood glucose assays were performed in the local physician practices. In addition, we did not have information concerning diabetes mellitus diagnoses at baseline, or about use of medications that might have affected blood glucose levels. This may have biased estimates toward the null for the highest level of glucose exposure. Therefore, the true estimates in the category ≥7.0 mmol/l may be even higher than the observed values. For high-normal blood glucose (5.3–6.0 mmol/l) and impaired fasting glycaemia (6.1–6.9 mmol/l) non-differential misclassification could have biased the hazard ratios upwards [38], but not beyond the true (unbiased) effect of the highest level of fasting glucose [39].
The proportion of cohort participants with blood glucose levels ≥7.0 mmol/l (3.4%) was somewhat low relative to Korean Cancer Prevention Study participants (approximately 4.2%) and expectations based on the estimated prevalence of adult diabetic patients in developed countries (5.9%) [40]. The prevalence of current and former smokers was comparable to a previous cross-sectional study of Austrians [41]; however, about 34% of lung cancers in our cohort were diagnosed in participants classified as never smokers, which suggests some misclassification of smoking status. In the statistical analysis we controlled for BMI and used occupational group as a rough surrogate for socioeconomic status but were unable to account for other factors that might have confounded relations between blood glucose and specific cancers, such as physical activity or diet.
In summary, our results provide further evidence of a positive association between hyperglycaemia and all cancers combined. Positive associations were also found for liver cancer and non-Hodgkin’s lymphoma in men; for colorectal, breast and bladder cancers in women, and for multiple myeloma, gallbladder/bile duct cancer, and thyroid cancer in men and women combined. Finally, our results indicate that fasting blood glucose values in the upper normal range, as well as values consistent with impaired fasting glycaemia and diabetes, may increase the risks of several types of cancer.
Abbreviations
- DCO:
-
death certificate only
- HR:
-
hazard rate ratio
- IARC:
-
International Agency for Research on Cancer
- VHM&PP:
-
Vorarlberg Health Monitoring and Promotion Programme
- WHO:
-
World Health Organization
References
Wideroff L, Gridley G, Mellemkjaer L et al (1997) Cancer incidence in a population-based cohort of patients hospitalized with diabetes mellitus in Denmark. J Natl Cancer Inst 89:1360–1365
Coughlin SS, Calle EE, Teras LR, Petrelli J, Thun MJ (2004) Diabetes mellitus as a predictor of cancer mortality in a large cohort of US adults. Am J Epidemiol 159:1160–1167
La Vecchia C, Negri E, Franceschi S, D’Avanzo B, Boyle P (1994) A case-control study of diabetes mellitus and cancer risk. Br J Cancer 70:950–953
Adami HO, McLaughlin J, Ekbom A et al (1991) Cancer risk in patients with diabetes mellitus. Cancer Causes Control 2:307–314
Ragozzino M, Melton LJ III, Chu CP, Palumbo PJ (1982) Subsequent cancer risk in the incidence cohort of Rochester, Minnesota, residents with diabetes mellitus. J Chronic Dis 35:13–19
Will JC, Galuska DA, Vinicor F, Calle EE (1998) Colorectal cancer: another complication of diabetes mellitus? Am J Epidemiol 147:816–825
Hu FB, Manson JE, Liu S et al (1999) Prospective study of adult onset diabetes mellitus (type 2) and risk of colorectal cancer in women. J Natl Cancer Inst 91:542–547
Weiderpass E, Gridley G, Nyren O, Ekbom A, Persson I, Adami HO (1997) Diabetes mellitus and risk of large bowel cancer. J Natl Cancer Inst 89:660–661
Adami HO, Chow WH, Nyren O et al (1996) Excess risk of primary liver cancer in patients with diabetes mellitus. J Natl Cancer Inst 88:1472–1477
Schoen RE, Tangen CM, Kuller LH et al (1999) Increased blood glucose and insulin, body size, and incident colorectal cancer. J Natl Cancer Inst 91:1147–1154
Muti P, Quattrin T, Grant BJ et al (2002) Fasting glucose is a risk factor for breast cancer: a prospective study. Cancer Epidemiol Biomarkers Prev 11:1361–1368
Manjer J, Kaaks R, Riboli E, Berglund G (2001) Risk of breast cancer in relation to anthropometry, blood pressure, blood lipids and glucose metabolism: a prospective study within the Malmo Preventive Project. Eur J Cancer Prev 10:33–42
Mink PJ, Shahar E, Rosamond WD, Alberg AJ, Folsom AR (2002) Serum insulin and glucose levels and breast cancer incidence: the atherosclerosis risk in communities study. Am J Epidemiol 156:349–352
Hsing AW, Gao YT, Chua S Jr, Deng J, Stanczyk FZ (2003) Insulin resistance and prostate cancer risk. J Natl Cancer Inst 95:67–71
Balkau B, Barrett-Connor E, Eschwege E, Richard JL, Claude JR, Ducimetiere P (1993) Diabetes and pancreatic carcinoma. Diabet Metab 19:458–462
Gapstur SM, Gann PH, Lowe W, Liu K, Colangelo L, Dyer A (2000) Abnormal glucose metabolism and pancreatic cancer mortality. JAMA 283:2552–2558
Levine W, Dyer AR, Shekelle RB, Schoenberger JA, Stamler J (1990) Post-load plasma glucose and cancer mortality in middle-aged men and women. 12-year follow-up findings of the Chicago Heart Association Detection Project in Industry. Am J Epidemiol 131:254–262
Saydah SH, Loria CM, Eberhardt MS, Brancati FL (2003) Abnormal glucose tolerance and the risk of cancer death in the United States. Am J Epidemiol 157:1092–1100
Batty GD, Shipley MJ, Marmot M, Smith GD (2004) Diabetes status and post-load plasma glucose concentration in relation to site-specific cancer mortality: findings from the original Whitehall study. Cancer Causes Control 15:873–881
Tulinius H, Sigfusson N, Sigvaldason H, Bjarnadottir K, Tryggvadottir L (1997) Risk factors for malignant diseases: a cohort study on a population of 22,946 Icelanders. Cancer Epidemiol Biomarkers Prev 6:863–873
Jee SH, Ohrr H, Sull JW, Yun JE, Ji M, Samet JM (2005) Fasting serum glucose level and cancer risk in Korean men and women. JAMA 293:194–202
Ulmer H, Kelleher C, Diem G, Concin H (2004) Why Eve is not Adam: prospective follow-up in 149650 women and men of cholesterol and other risk factors related to cardiovascular and all-cause mortality. J Womens Health (Larchmt) 13:41–53
Reinauer H, Home PD, Kanagasabapathy AS, Heuck C-C, World Health Organization (2002) Laboratory diagnosis and monitoring of diabetes mellitus. World Health Organization, Geneva
Parkin DM, Whelan SL, Ferlay J, Teppo L, Thomas DB, and all at the International Agency for Research on Cancer, Lyon France (2003) Cancer incidence in five continents, vol VIII, ISBN 92832 21559
Oberaigner W, Concin H, and Mathis G (2003) aks Report, vol 2; http://www.aks.or.at/berichte
WHO (2000) Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organization Technical Report Series 894:i–253
Macinnis RJ, English DR, Gertig DM, Hopper JL, Giles GG (2004) Body size and composition and risk of postmenopausal breast cancer. Cancer Epidemiol Biomarkers Prev 13:2117–2125
Rapp K, Schroeder J, Klenk J et al (2005) Obesity and incidence of cancer: a large cohort study of over 145 000 adults in Austria. Br J Cancer 93:1062–1067
Ish-Shalom D, Christoffersen CT, Vorwerk P et al (1997) Mitogenic properties of insulin and insulin analogues mediated by the insulin receptor. Diabetologia 40(Suppl 2):S25–S31
Khandwala HM, McCutcheon IE, Flyvbjerg A, Friend KE (2000) The effects of insulin-like growth factors on tumorigenesis and neoplastic growth. Endocr Rev 21:215–244
Calle EE, Kaaks R (2004) Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer 4:579–591
Davila JA, Morgan RO, Shaib Y, McGlynn KA, El Serag HB (2005) Diabetes increases the risk of hepatocellular carcinoma in the United States: a population based case control study. Gut 54:533–539
Angulo P (2002) Nonalcoholic fatty liver disease. N Engl J Med 346:1221–1231
Hjalgrim H, Frisch M, Ekbom A, Kyvik KO, Melbye M, Green A (1997) Cancer and diabetes – a follow-up study of two population-based cohorts of diabetic patients. J Intern Med 241:471–475
Natazuka T, Manabe Y, Kono M, Murayama T, Matsui T, Chihara K (1994) Association between non-insulin dependent diabetes mellitus and non-Hodgkin’s lymphoma. BMJ 309:1269
Kantor AF, Hartge P, Hoover RN, Narayana AS, Sullivan JW, Fraumeni JF Jr (1984) Urinary tract infection and risk of bladder cancer. Am J Epidemiol 119:510–515
La Vecchia C, Negri E, D’Avanzo B, Savoldelli R, Franceschi S (1991) Genital and urinary tract diseases and bladder cancer. Cancer Res 51:629–631
Dosemeci M, Wacholder S, Lubin JH (1990) Does nondifferential misclassification of exposure always bias a true effect toward the null value? Am J Epidemiol 132:746–748
Correa-Villasenor A, Stewart WF, Franco-Marina F, Seacat H (1995) Bias from nondifferential misclassification in case-control studies with three exposure levels. Epidemiology 6:276–281
King H, Aubert RE, Herman WH (1998) Global burden of diabetes, 1995–2025: prevalence, numerical estimates, and projections. Diabetes Care 21:1414–1431
Ulmer H, Diem G, Bischof HP, Ruttmann E, Concin H (2001) Recent trends and sociodemographic distribution of cardiovascular risk factors: results from two population surveys in the Austrian WHO CINDI demonstration area. Wien Klin Wochenschr 113:573–579
Acknowledgements
We thank all the physicians and participants in the Vorarlberg Health Monitoring and Promotion Programme (VHM&PP) for completing the study examinations and for providing data. The VHM&PP is supported by the State of Vorarlberg, Austria.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rapp, K., Schroeder, J., Klenk, J. et al. Fasting blood glucose and cancer risk in a cohort of more than 140,000 adults in Austria. Diabetologia 49, 945–952 (2006). https://doi.org/10.1007/s00125-006-0207-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-006-0207-6