
Abstract
Aims/hypothesis
The largely unsatisfactory results reported for the pharmacological treatment of diabetic neuropathy has spurred the search for alternative therapies. The aim of this study was to evaluate the efficacy of frequency-modulated electromagnetic neural stimulation (FREMS) as a novel treatment for painful diabetic neuropathy.
Methods
Patients (n=31) with painful neuropathy associated with decreased nerve conduction velocity (<40 m/s) and increased vibration perception threshold (>25 V) were enrolled in a randomised, double-blind, crossover study designed to compare the effects of FREMS with those of placebo. Each patient received two series of ten treatments of either FREMS or placebo in random sequence, with each series lasting no more than 3 weeks. The primary efficacy end point was the change in pain measured by a visual analogue scale (VAS).
Results
FREMS induced a significant reduction in daytime and night-time VAS pain score (all p<0.02). Furthermore, FREMS induced a significant increase in sensory tactile perception, as assessed by monofilament; a decrease in foot vibration perception threshold, as measured by a biothesiometer; and an increase in motor nerve conduction velocity (all p<0.01). No significant changes were observed after placebo. Comparison of measurements at the 4-month follow-up with those at baseline revealed that a significant benefit persisted for all measures that showed an improvement at the end of treatment, with an additional improvement in quality of life evaluated by the Short Form-36 questionnaire (all p<0.05). No significant side effects were recorded during the study.
Conclusions/interpretation
FREMS is a safe and effective therapy for neuropathic pain in patients with diabetes and is able to modify some parameters of peripheral nerve function.
Similar content being viewed by others


Introduction
Peripheral neuropathy is a frequent and disabling microvascular complication of both type 1 and type 2 diabetes [1]. This condition may be prevented by good blood glucose control [2]; however, it is at best halted, once established, even after long-term blood glucose normalisation, such as that observed following successful pancreas transplantation [3, 4]. The pathological hallmarks of diabetic neuropathy are microangiopathy of the vasa nervorum, loss of axons and axonal atrophy, all of which are the result of a combination of different mechanisms of tissue damage that are common to all long-term complications of diabetes [5].
The pharmacological treatment of diabetic neuropathy is largely unsatisfactory, mainly due to a lack of drugs that act on the underlying pathogenetic mechanisms. Aldose reductase inhibitors are among the few compounds with this mode of action; however, the results of clinical trials performed to date have been disappointing [6]. Consequently, current therapy is purely symptomatic, aiming to relieve the pain associated with neuropathy through the administration of various analgesics, tricyclic antidepressants, anti-arrhythmics [7] and, more recently, the new anti-epileptic agents gabapentin [8] and lamotrigine [9], and opioids [10].
Non-pharmacological symptomatic treatments have also been proposed, including acupuncture [11], near-infrared phototherapy [12], low-intensity laser therapy [13], static and pulsed magnetic field therapies [14, 15], and various electrotherapies, including transcutaneous electrical nerve stimulation (TENS) [16, 17], percutaneous electrical nerve stimulation [18] and spinal cord electrostimulation [19]. The rationale for the use of electrical nerve stimulation in diabetic neuropathy is based on its historical, though controversial, use in various painful clinical conditions [20] and on some beneficial effects reported in the treatment of other diabetic complications, such as foot ulcers [21].
Frequency-modulated electromagnetic neural stimulation (FREMS) has recently been developed as a novel electrotherapy. This method is different from TENS and other known electrotherapy systems, as it uses sequences of modulated electrical stimuli that vary automatically in terms of pulse frequency, duration and voltage amplitude. The FREMS method was designed on the basis of the hypothesis that the summation of sub-threshold electrical stimuli, conveyed through the skin proximal to a motor nerve in a non-invasive system, would induce composite motor action potentials in excitable tissues. A single impulse of low intensity and short duration, such as that used by conventional electrotherapies, is unable to overcome the dielectric skin barrier to excite the underlying nervous or muscular tissue. However, FREMS achieves this effect through specific sequences of weak impulses, characterised by a rapid increase and decrease in pulse frequency and duration, which result in the gradual recruitment of membrane potentials in the stimulated tissues [22].
These characteristics prompted us to evaluate the therapeutic potential of FREMS in human diabetic neuropathy. In this paper we report the results of a two-centre, randomised, double-blind, placebo-controlled, crossover clinical trial on FREMS treatment of patients with painful diabetic neuropathy.
Subjects and methods
Study design and end points
The study had a randomised, double-blind, placebo-controlled, crossover design. The primary end point was the change in grading of daytime and night-time pain, as assessed using a visual analogue scale (VAS). Secondary end points were changes in: sensitivity to monofilament; vibration perception threshold, as measured by a biothesiometer; quality of life, as assessed by questionnaire; motor nerve conduction velocity (MNCV); and sensory nerve conduction velocity (SNCV). The treatment consisted of ten sessions of placebo followed by ten sessions of FREMS (sequence 1) or vice versa (sequence 2) at random, separated by a wash-out period of 1 week. Each treatment session was administered at intervals of at least 24 h, and each ten-session series lasted no more than 3 weeks. Randomisation to sequence 1 or sequence 2 was performed centrally at the time of enrolment. Principal investigators, physicians, nurses, technicians and statisticians were unaware of treatment assignment.
Characteristics of FREMS
Treatment with FREMS was performed using sequences of monophase-compensated negative potential electrical pulses that are characterised by a sharp spike and an asymmetrical shape (peak amplitude variable from 0–255 V, pulse frequency variable within the range 1–50 Hz, pulse duration variable within the range 10–40 μs).
Administration of FREMS and placebo
Electrotherapy and placebo were administered using the Physioflog ETS 501 (Lorenz Therapy System; Lorenz Biotech, Medolla, Italy) via four electrodes applied to the lower extremities; the original device was modified by the addition of a switch to apply treatment A (later revealed to be placebo) or treatment B (later revealed to be FREMS). Each session of either placebo or FREMS lasted for 30 min. Placebo consisted of no electric current transmission. This placebo was chosen after a preliminary study had shown that patients with a vibration perception threshold higher than 25 V effectively had no perception of the electrical stimuli administered by the FREMS device (data not shown). These findings were in accordance with those reported by two other studies showing a direct correlation between vibration perception threshold measured by a biothesiometer and current perception threshold measured by a Neurometer (Neurotron, Baltimore, MD, USA) across the same range of frequencies used by FREMS [23, 24]. During sessions of either placebo or FREMS, patients were invited to modulate the delivery of neurostimulation themselves, by progressively increasing the voltage of electrical stimulation along a scale of 0–255 V through a manually gradable remote control device that increased the voltage by 1 V per step up to the maximal allowed, which corresponded to the possible perception of burning at the site of the electrode.
Subjects
Patients who met the following criteria were invited to participate in the study: (1) type 1 or type 2 diabetes according to American Diabetes Association criteria [25]; (2) age between 18 and 70 years; (3) painful diabetic neuropathy with reduced sensory and/or MNCV (<40 m/s in at least one nerve trunk of lower limbs); and (4) vibration perception at big toe >25 V. Exclusion criteria were: (1) the presence of any other severe disease; (2) pregnancy; (3) renal disease with serum creatinine levels >1.77 μmol/l; (4) a history or actual presence of foot ulcers; and (5) lower limb vasculopathy as indicated by an ankle-brachial index <0.9 or a transcutaneous partial pressure of oxygen <50 mmHg. Any analgesic or other drug administered for the chronic treatment of painful neuropathy was discontinued at least 3 weeks before randomisation. Patients were enrolled at two centres: Milan and Perugia. The study protocol was approved by the ethics committees of San Raffaele University Hospital and Perugia University Hospital, and written informed consent was obtained from all patients prior to enrolment.
Clinical assessments
Patients were evaluated four times: at baseline, at the end of each series, and 4 months after the completion of the study. Each patient saw the same physician for the clinical examination, the administration of questionnaires and the assessment of side effects; two neurophysiologists, one in Milan and one in Perugia, performed electroneurography examinations.
Outcome measures
The parameters described below were measured on four occasions. Daytime and night-time pain were measured by a 0–100 VAS (results expressed as absolute numbers) [26]. Tactile sensation was assessed by the 5.07 (10 g) Semmes–Weinstein monofilament test (the number of insensitive areas in the two feet out of nine standard areas per foot—the first, third and fifth finger and respective metatarsal heads, two mid-foot points and heel—are assessed; only data for the right foot were considered for analysis) [27]. Foot vibration perception threshold was measured using a biothesiometer (Bio-Medical Instrument Company, Newbury, OH, USA) [28]. Electroneurography was used to measure MNCV and SNCV in m/sec according to the standard procedure [29]; a Micromed System 98 was used in Milan (Myoquick, Treviso, Italy), whereas a Medelec Premier Plus (TECA, NY, USA) was used in Perugia. MNCV was measured in the peroneal nerve and SNCV was measured antidromically in the sural nerve. Quality of life was assessed using the Short Form-36 questionnaire (SF36) [30]. The SF36, which was originally used to assess health status in the Medical Outcomes Study, was calculated on a total of 142 levels, where the highest score represents the highest quality of life. The scale covers the following eight domains: general health; physical functioning; role limitation due to physical and social functioning; social functioning; bodily pain; general mental health; role limitation due to emotional problems; and vitality. HbA1c was measured locally by ionic exchange HPLC (Variant 2; Biorad, Milan, Italy) at baseline and at the end of the two treatment series.
Statistical analysis
The ANOVA test for repeated measures was used to analyse changes in all variables. A Neuman–Keuls multiple comparison test was used in post-test analyses. A crossover model was used to evaluate both the carryover and treatment effects [31]. A paired t-test was used to analyse the changes in all variables during FREMS or placebo. Descriptive statistics are reported as means±SE. Comparison of the effects of FREMS with those of placebo were made using all FREMS and placebo series. In addition, the effect of FREMS at 4-month follow-up was analysed by comparison with baseline values. A p value less than 0.05 was considered statistically significant.
Results
Subjects
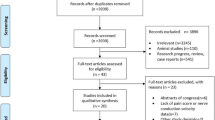
Between October 2001 and December 2003, 38 patients were screened and 31 were enrolled in the study and randomised to sequence 1 or sequence 2. The characteristics of the two sequence assignment groups were not significantly different at baseline (Table 1). MNCV was measured in 26 patients and SNCV was measured in 15 patients, due to unrecordable nerve action potentials in the remainder, and the results of the Semmes–Weinstein monofilament test were only recorded for the 12 patients enrolled in Milan. Data analysis was based on 31 patients for all other measures. Although no specific attempts were made to improve diabetes control during the study, HbA1c significantly decreased from baseline to the end of FREMS and placebo sequences (8.5±0.3 vs 7.9±0.2%, p=0.001), most likely as a trial effect.
Efficacy
Within-treatment analysis showed that, following FREMS treatment, there was a significant decrease in daytime pain score (p=0.0025) and night-time pain score (p=0.0107), a significant decrease in the number of points insensitive to the Semmes–Weinstein monofilament (p=0.0077), a significant decrease in the vibration perception threshold (p=0.0001), and a significant increase in MNCV (p=0.0019). Non-significant trends towards improvements in quality of life and SNCV were also observed after FREMS. None of the outcome measures changed significantly during treatment with placebo (Table 2). No carryover effect was evident within the crossover analysis.
When compared with baseline measurements, the results of the 4-month follow-up showed the persistence of statistically significant changes in all the parameters modified by FREMS during treatment, including: daytime pain score (p<0.01); night-time pain score (p<0.01); vibration perception threshold (p<0.05); sensory perception, as assessed by monofilament (p<0.001); and MNCV (p<0.05). In addition, significant improvements were observed for overall quality of life (p<0.001); the domains for which significant improvements were observed were bodily pain, social functioning, physical functioning, role limitation to physical and social functioning, and general mental health (all p<0.05), while no significant improvement was shown in general health perception, role limitation to emotional problems, or vitality (Table 3). A non-significant trend towards improvement of SNCV was also observed.
Safety
No systemic side effects were recorded during the study. Patients reported only a very slight burning sensation at the site of electrode placement during the series of treatments later revealed as FREMS, with no residual skin signs. No particular perception was recorded during placebo sessions.
Discussion
We have demonstrated that FREMS is a safe and effective therapy for neuropathic pain in diabetic patients with peripheral neuropathy and that it is able to modify some of the parameters of peripheral nerve function. The results of our two-centre, randomised, double-blind, placebo-controlled, crossover clinical trial show that the beneficial effect of FREMS is superior to any placebo influence.
Therapy for neuropathic pain is generally based on analgesic drugs, but the frequency of side effects and the lack of efficacy of these agents in a significant proportion of cases has spurred the search for non-pharmacological treatments. FREMS is significantly different from other known electrotherapy systems because of the modulation of the frequency, amplitude and duration of the electrical stimuli. At the end of FREMS sessions, we observed a significant reduction of pain (up to −29% for daytime pain and −25% for night-time pain as measured by a VAS). As expected, some pain reduction was also observed after placebo, although the reduction was only statistically significant after FREMS. This non-invasive treatment was demonstrated to be safe and was not associated with any side effects. Although the study was blind, patients reported some perceptions at the site of electrode placement during several sessions of the treatment later revealed as FREMS; this did not happen during sessions later revealed as placebo. However, it is unlikely that these subjective perceptions influenced the study, since neither the patients nor the investigators were aware of whether the placebo was a nonsense electrical stimulation or a lack of stimulation. At most, only a marginal influence on some of the less objective measures, such as tactile or vibration perceptions, might be hypothesised. Our results also demonstrate that the efficacy of FREMS is maintained for at least 4 months, as both daytime and night-time pain remained significantly reduced compared with baseline at the 4-month follow-up. This finding could be specific to FREMS, since none of the non-pharmacological treatments for painful diabetic neuropathy investigated to date have reported a beneficial effect lasting for more than a few weeks. Our results add to increasing evidence suggesting that non-pharmacological tools may be useful in the treatment of neuropathic pain. Of these modalities, FREMS could be particularly advantageous in terms of effect duration.
In our study, in addition to its analgesic effect, FREMS was shown to improve several other functional peripheral nerve parameters. On average, at the end of active treatment, MNCV was increased by almost 5 m/s; vibration perception threshold, as measured by a biothesiometer, was reduced by more than 2 V; and the number of foot points insensitive to the Semmes–Weinstein monofilament was decreased by 1.2. Although the monofilament observation is limited by the small number of patients assessed, these findings demonstrate that peripheral nerve function is ameliorated after treatment with FREMS. It is unlikely that these findings are the result of the observed improvement in blood glucose control, indicated by the significant decrease in HbA1c during the study. As demonstrated by the Diabetes Control and Complications Trial [2] and in studies on pancreas transplant patients [3, 4], strict glucose control is able to prevent or halt the progression of an already established peripheral neuropathy. However, such effects are seen over a long period of time, whereas in this study the symptomatic improvement induced by FREMS was measurable during the 3 weeks of active treatment.
The extent to which the MNCV increased during the study was remarkable: a ∼5-m/s increase was observed at the end of FREMS treatment and a >3-m/s increase was maintained at the 4-month follow-up. A meta-analysis of clinical studies using aldose reductase inhibitors, which included 19 clinical trials using four different drugs, reported a reduction of 0.53 m/s in the rate of decrease of peroneal nerve conduction velocity over a median period of 6 months [32]. According to our results, FREMS appears to be superior to these pharmacological agents. Furthermore, the improvement obtained after FREMS is greater than 2.2 m/s, the value indicated by the Peripheral Nerve Society as the minimal increase in peroneal nerve conduction velocity at which clinical amelioration can be appreciated [33].
The mechanism of action of FREMS was not investigated in this study, and can therefore only be speculated upon. Based on a number of assumptions, an attractive hypothesis is that FREMS stimulates the release of vasoactive factors, which results in an increase in endoneural blood flow, thus reversing the endoneural microvessel disease and associated nerve hypoxia. Indirect findings that may be related to the effects of FREMS include: (1) the induction of the synthesis of vascular endothelial growth factor (VEGF) and other angiogenic factors and angiogenesis promotion by different electrical [34–36] or electromagnetic [37] stimuli; (2) the reversal of diabetic neuropathy in an experimental model by VEGF gene transfer [38]; (3) increased conduction velocity mediated by an increase in endoneural blood flow after electrical stimulation of peripheral nerves in a model of experimental diabetic neuropathy [39]; and (4) increased nerve conduction velocity after an improvement in blood flow in the lower limbs, achieved through either revascularisation [40] or physical exercise [41]. Alternatively, FREMS might act on neuron sodium channels. Recent evidence suggests that sodium channel expression in primary sensory neurons is altered in diabetic neuropathy [42], indicating a possible molecular basis for neuropathic pain. Given the evidence that exogenous electric fields induce cellular responses that involve the redistribution of integral membrane proteins, including calcium channels [43], a similar effect on sodium channels may be hypothesised. It is noteworthy that the subjects enrolled in our study were affected by relatively severe neuropathy, which is normally associated with a decrease in the number of myelin fibres and altered endoneural vessels. Thus, it is likely that the observed improvements in MNCV and vibration perception threshold at the end of FREMS treatment simply reflect some functional changes of the nerve; structural changes may only occur at a later stage, possibly providing the basis for the long-term effects of this therapy. Nonetheless, studies on experimental models of neuropathy are needed in order to clarify the mechanisms that underlie the effects of FREMS.
In conclusion, the results of this controlled clinical trial demonstrate the analgesic efficacy of FREMS, and show additional beneficial effects of this novel electrotherapy on peripheral nerve function in patients with peripheral diabetic neuropathy. If confirmed in a larger series of cases, and possibly in a multicentre study, these findings may offer new perspectives for the treatment of diabetic neuropathy.
Abbreviations
- FREMS:
-
frequency-modulated electromagnetic neural stimulation
- MNCV:
-
motor nerve conduction velocity
- SF36:
-
Short Form-36 questionnaire
- SNCV:
-
sensory nerve conduction velocity
- TENS:
-
transcutaneous electrical nerve stimulation
- VAS:
-
visual analogue scale
- VEGF:
-
vascular endothelial growth factor
References
Vinik AI, Park TS, Stansberry KB, Pittenger GL (2000) Diabetic neuropathies. Diabetologia 43:957–973
DCCT/EDIC Research Group (2002) Effect of intensive therapy on the microvascular complications of type 1 diabetes mellitus. JAMA 287:2563–2569
Martinenghi S, Comi G, Galardi G, Di Carlo V, Pozza G, Secchi A (1997) Amelioration of nerve conduction velocity following simultaneous kidney/pancreas transplantation is due to the glycaemic control provided by the pancreas. Diabetologia 40:1110–1112
Navarro X, Sutherland DER, Kennedy WR (1997) Long-term effects of pancreatic transplantation on diabetic neuropathy. Ann Neurol 42:727–736
Brownlee M (2001) Biochemistry and molecular cell biology of diabetic complications. Nature 414:813–820
Pfeifer MA, Schumer MP, Gelber DA (1997) Aldose reductase inhibitors: the end of an era or the need for different trial designs? Diabetes 46(Suppl 2):S82–S89
Benbow SJ, Cossins L, MacFarlane IA (1999) Painful diabetic neuropathy. Diabet Med 16:632–644
Backonja M, Beydoun A, Edwards KR et al (1998) Gabapentin for the symptomatic treatment of painful neuropathy in patients with diabetes mellitus: a randomized controlled trial. JAMA 280:1831–1836
Eisenberg E, Lurie Y, Braker C, Daoud D, Ishay A (2001) Lamotrigine reduces painful diabetic neuropathy: a randomized, controlled study. Neurology 57:505–509
Watson CP, Moulin D, Watt-Watson J, Gordon A, Eisenhoffer J (2003) Controlled-release oxycodone relieves neuropathic pain: a randomized controlled trial in painful diabetic neuropathy. Pain 105:71–78
Abuaisha BB, Costanzi JB, Boulton AJ (1998) Acupuncture for the treatment of chronic painful peripheral diabetic neuropathy: a long-term study. Diabetes Res Clin Pract 39:115–121
Leonard DR, Farooqi MH, Myers S (2004) Restoration of sensation, reduced pain, and improved balance in subjects with diabetic peripheral neuropathy. A double-blind, randomized, placebo-controlled study with monochromatic near-infrared treatment. Diabetes Care 27:168–172
Zinman L, Ngo M, Ng ET, Nwe KT, Gogov S, Bril V (2004) Low-intensity laser therapy for painful symptoms of diabetic sensorimotor polyneuropathy. A controlled trial. Diabetes Care 27:921–924
Weintraub MI, Wolfe GI, Barohn RA et al (2003) Static magnetic field therapy for symptomatic diabetic neuropathy: a randomized, double-blind, placebo-controlled trial. Arch Phys Med Rehabil 84:736–746
Weintraub MI, Cole SP (2004) Pulsed magnetic field therapy in refractory neuropathic pain secondary to peripheral neuropathy: electrodiagnostic parameters—pilot study. Neurorehabil Neural Repair 18:42–46
Kumar D, Marshall HJ (1997) Diabetic peripheral neuropathy: amelioration of pain with transcutaneous electrostimulation. Diabetes Care 20:1702–1705
Kumar D, Alvaro MS, Julka IS, Marshall HJ (1998) Diabetic peripheral neuropathy. Effectiveness of electrotherapy and amitriptyline for symptomatic relief. Diabetes Care 21:1322–1325
Hamza MA, White PF, Craig WF et al (2000) Percutaneous electrical nerve stimulation: a novel analgesic therapy for diabetic neuropathic pain. Diabetes Care 23:365–370
Tesfaye S, Watt J, Benbow SJ, Pang KA, Miles J, MacFarlane IA (1996) Electrical spinal-cord stimulation for painful diabetic peripheral neuropathy. Lancet 348:1698–1701
Neumann V (1993) Electrotherapy. Br J Rheumatol 32:1–2
Baker LL, DeMuth SK, Chambers R, Villar F (1997) Effects of electrical stimulation on wound healing in patients with diabetic ulcers. Diabetes Care 20:405–412
Bevilacqua M, Barrella M, Toscano R et al (2004) Disturbances of vasomotion in diabetic (type 2) neuropathy: increase of vascular endothelial growth factor, elicitation of sympathetic efflux and synchronization of vascular flow (vasomotion) during frequency modulated neural stimulation (FREMS). 86th Annual Meeting of the Endocrine Society, p 321, P 2–61 (abstract)
Donague VM, Giurini JM, Rosenblum BI, Weissman PN, Veves A (1995) Variability in function measurements of three sensory foot nerves in neuropathic diabetic patients. Diabetes Res Clin Pract 29:37–42
Pitei DL, Watkins PJ, Stevens MJ, Edmonds ME (1994) The value of the Neurometer in assessing diabetic neuropathy by measurement of the current perception threshold. Diabet Med 11:872–876
Genuth S, Alberti KG, Bennett P et al (2003) Expert committee on the diagnosis and classification of diabetes mellitus. Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care 26:3160–3167
Ohnhaus EE, Adler R (1975) Methodological problems in the measurement of pain: a comparison between the verbal rating scale and the visual analogue scale. Pain 1:379–384
Kumar S, Fernando DJ, Veves A, Knowles EA, Young MJ, Boulton AJ (1991) Semmes–Weinstein monofilaments: a simple, effective and inexpensive screening device for identifying diabetic patients at risk of foot ulceration. Diabetes Res Clin Pract 13:63–67
Bloom S, Till S, Sonksen P, Smith S (1984) Use of a biothesiometer to measure individual vibration thresholds and their variation in 519 non-diabetic subjects. Br Med J 288:1793–1795
Preston DC, Shapiro BE (1998) Electromyography and neuromuscular disorders. Butterworth-Heinemann, Boston, pp 103–142
Ware JE Jr, Sherbourne CD (1992) The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 30:473–483
Koch GG (1972) The use of non-parametric methods in the statistical analysis of the two-period change-over design. Biometrics 28:577–584
Airey M, Bennett C, Nicolucci A, Williams R (2000) Aldose reductase inhibitors for the prevention and treatment of diabetic peripheral neuropathy. Cochrane Database Syst Rev CD002182
Peripheral Nerve Society (1995) Diabetic polyneuropathy in controlled clinical trials: consensus report of the Peripheral Nerve Society. Ann Neurol 38:478–482
Zhao M, Bai H, Wang E, Forrester JV, McCaig CD (2004) Electrical stimulation directly induces pre-angiogenic responses in vascular endothelial cells by signaling through VEGF receptors. J Cell Sci 117:397–405
Hang J, Kong L, Gu JW, Adair TH (1995) VEGF gene expression is upregulated in electrically stimulated rat skeletal muscle. Am J Physiol 269:H1827–H1831
Kanno S, Oda N, Abe M et al (1999) Establishment of a simple and practical procedure applicable to therapeutic angiogenesis. Circulation 99:2682–2687
Tepper OM, Callaghan MJ, Chang EI et al (2004) Electromagnetic fields increase in vitro and in vivo angiogenesis through endothelial release of FGF-2. FASEB J 18:1231–1233
Schratzberger P, Walter DH, Rittig K et al (2001) Reversal of experimental diabetic neuropathy by VEGF gene transfer. J Clin Invest 107:1083–1092
Cameron NE, Cotter MA, Robertson S, Maxfield EK (1993) Nerve function in experimental diabetes in rats: effects of electrical stimulation. Am J Physiol 264:E161–E166
Young MJ, Veves A, Smith JV, Walker MG, Boulton AJM (1995) Restoring lower limb blood flow improves conduction velocity in diabetic patients. Diabetologia 38:1051–1054
Tesfaye S, Harris ND, Wilson RM, Ward JD (1992) Exercise-induced conduction velocity increment: a marker of impaired peripheral nerve blood flow in diabetic neuropathy. Diabetologia 35:155–159
Craner MJ, Klein JP, Renganathan M, Black JA, Waxman SG (2002) Changes of sodium channel expression in experimental painful diabetic neuropathy. Ann Neurol 52:786–792
Cho MR, Thatte HS, Silvia MT, Golan DE (1999) Transmembrane calcium influx induced by ac electric fields. FASEB J 13:677–683
Acknowledgements
This study was supported in part by a research grant from Lorenz Biotech (Medolla, Italy). The funding company had no role in the design and conduct of the study, the analysis and interpretation of the data, or in the preparation and review of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bosi, E., Conti, M., Vermigli, C. et al. Effectiveness of frequency-modulated electromagnetic neural stimulation in the treatment of painful diabetic neuropathy. Diabetologia 48, 817–823 (2005). https://doi.org/10.1007/s00125-005-1734-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-005-1734-2