
Abstract
Aims/hypothesis
Moderate alcohol intake has been associated with increased life expectancy due to reduced mortality from cardiovascular disease. We prospectively examined the effects of alcohol consumption on mortality in Type 2 diabetic patients in Switzerland.
Methods
A total of 287 patients with Type 2 diabetes mellitus (125 women, 162 men), recruited in Switzerland for the WHO Multinational Study of Vascular Disease in Diabetes, were included in this study. After a follow-up period of 12.6±0.6 years (means ± SD), mortality from CHD and from all causes was assessed.
Results
During the follow-up, 70 deaths occurred (21 from CHD, 49 from other causes). Compared with non-drinkers, alcohol consumers who drank alcohol 1 to 15 g, 16 to 30 g and 30 g or more per day had the following risk rates of death from CHD: 0.87 (95% CI: 0.25 to 2.51, NS), 0.00 (95% CI: 0.00 to 0.92, p less than 0.05) and 0.37 (95% CI, 0.01 to 2.42, NS), respectively. The corresponding risk rates of death from all causes were 1.27 (95% CI: 0.68 to 2.28, NS), 0.36 (95% CI: 0.09 to 0.99, p less than 0.05) and 1.66 (95% CI: 0.76 to 3.33, NS).
Conclusions/interpretation
In Swiss Type 2 diabetic patients moderate alcohol consumption of 16 to 30 g per day was associated with reduced mortality from CHD and from all causes. Alcohol intake above 30 g per day was associated with a tendency towards increased all-cause mortality.
Similar content being viewed by others

Light to moderate alcohol consumption lowers the risk of CHD and has been associated with increased life expectancy due to reduced cardiovascular mortality [1, 2, 3, 4, 5]. The benefit of light to moderate alcohol intake could be highest in people at increased risk of CHD [4, 6]. Most published data demonstrating a cardio-protective effect of alcohol consumption were obtained in mixed populations, including primarily non-diabetic subjects, and the proportion of diabetic patients included in these studies was not known. Recently the protective effect of light to moderate alcohol consumption on the risk of cardiovascular morbidity and mortality in patients with diabetes has been investigated [7, 8, 9, 10]. These studies confirmed the reduced mortality from CHD in female [8], male [9, 10] and mixed populations [7] of diabetic patients who drink alcohol, and are consistent with previous results in people without diabetes. All of these investigations were carried out in North America where drinking patterns [11] and type of alcoholic beverage are possibly different from those in other areas. Due to differences in the prevalence of cardiovascular risk factors and differences in ethnicity, a direct translation of results to other populations should be treated with caution.
The aim of our study was to find out whether results obtained in North American populations [7, 8, 9, 10] can be repeated in a well-defined, central European population representative for a whole country. We prospectively examined the relationship between self-reported alcohol consumption and death rates from CHD and from all causes in Type 2 diabetic patients who were members of the Swiss cohort of the WHO Multinational Study of Vascular Disease in Diabetes [12].
Subjects and methods
Study population
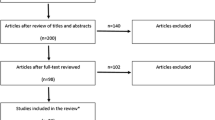
The Swiss cohort [12] of the WHO Multinational Study of Vascular Disease in Diabetes [13, 14] included 533 patients selected randomly, according to the central protocol, from the diabetic patients of 231 local practitioners from all over the country [12]. The sample was representative of a large area including almost the entire country. Patients were stratified according to sex, age and duration of diabetes as follows: sex: 255 women, 278 men; age: 35 to 41 years (34.0% women, 32.4% men), 42 to 48 years (34.8% women, 35.3% men), 49 to 55 years (31.3% women, 32.4% men); duration: 1 to 6 years (34.0% women, 34.5% men), 7 to 13 years (30.1% women, 32.0% men), over 13 years (35.9% women, 33.5% men).
Diabetes mellitus was diagnosed on a clinical basis. According to the central protocol [12, 13], a diabetic patient was defined as someone diagnosed at least 1 year earlier and receiving specific treatment for diabetes from a physician. All patients needing insulin treatment within 1 year of diagnosis were defined as having Type 1 diabetes [13]. The remaining patients were classified as Type 2 diabetic patients. Based on these definitions, 308 patients were identified as having Type 2 diabetes. For 287 patients with Type 2 diabetes (93.2%) data on self-reported alcohol consumption were available. Only these patients were included in our analysis. Thirteen patients left Switzerland and were lost for the final follow-up, but on all of them intermediary data were available and the day they left the country was provided by Federal authorities and their physicians. At baseline a standardised clinical examination was done, including a detailed questionnaire with information on diabetes diagnosis, duration and treatment, as well as on symptoms of vascular disease. In addition, height, weight and blood pressure were recorded. Urine was tested for proteinuria using the sulphosalicylic acid method. Venous blood was drawn to measure cholesterol and creatinine. A resting 12-lead electrocardiogram was recorded. These baseline investigations were done between February 1974 and May 1977. Analyses were carried out in accordance with the Declaration of Helsinki and the Swiss laws regarding data safety. Data used were made fully anonymous before the analyses and only aggregate are reported.
Alcohol consumption
At baseline, the self-reported consumption of alcoholic beverages was assessed and daily alcohol intake was calculated on the basis of weekly consumption of beer, wine and spirits. Depending on daily alcohol intake, four groups of patients were formed: group 1 with 0 g per day (non-drinkers); group 2 with 1 to 15 g per day; group 3 with 16 to 30 g per day; and group 4 with more than 30 g per day.
Follow-up and outcome definition
Life or death status was ascertained as per January 1st, 1988 after 12.6±0.6 years (means ± SD, 5543 person-years). During the follow-up 70 deaths were identified. In deceased patients the underlying cause of death was established from a copy of the death certificate, hospital records, post-mortem reports (where available) and from additional information given by the deceased persons' physicians. The underlying cause of death was coded according to the International Classification of Disease 9 (ICD-9) [15]. CHD included ICD codes 410 to 414.
Statistical analysis
Data analysis was done using Excel (Microsoft Corporation, Redmond, Wash., USA), Statview (SAS Institute, Cary, N.C., USA) and PEPI 4.0 (Computer Programs for Epidemiologists, Brixton Books, Llanidloes, UK). Data are given as means ± SD, as risk rates (RR) with a 95% CI or as incidence rates (rate per 1000 patient-years). Statistical assessment of differences between two or more groups was done using the two-tailed Student's t test or ANOVA as appropriate. Proportions and incidence rates were compared using Fisher's exact test. Survival analysis was done using Kaplan-Meier statistics and the Cox proportional hazards model. The Cox proportional hazards model was used to estimate the relative risk (and the 95% CI) associated with alcohol consumption and adjust it for other risk factors. Patients who left Switzerland were censored on the day they left the country. A p value of less than 0.05 was considered statistically significant.
Results
Patient characteristics (Table 1)
Baseline characteristics of patients who died, patients who survived and all patients combined are shown in Table 1. There were significant differences between patients who died, patients who survived with respect to age (p<0.001), systolic blood pressure (p<0.001), triglycerides (p=0.001) and creatinine (p=0.003). P values for sex distribution (p=0.096), duration of diabetes (p=0.053), diastolic blood pressure (p=0.076) and cholesterol (p=0.094) and fasting plasma glucose (p=0.079) did not quite reach statistical significance.
Alcohol consumption and mortality (Tables 2 and 3, Fig. 1)
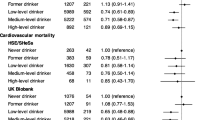
The self-reported consumption of alcoholic beverages and the calculated average daily alcohol intake was documented in all patients. A total of 153 patients (54 men, 99 women) consumed no alcoholic beverages (group 1, non-drinkers); 61 patients (46 men, 15 women) consumed 1 to 15 g per day (group 2); 42 patients (33 men, 9 women) consumed 16 to 30 g per day (group 3); and 31 patients (29 men, 2 women) consumed more than 30 g per day (group 4). During a follow-up of 12.6±0.6 years (5543 person-years) 70 patients (24.4%) died. In 21 patients death from CHD was documented. In 42 patients consuming 16 to 30 g alcohol per day no deaths from CHD were registered (for comparison with the non-drinker group a p value of 0.037 was considered to be significant). Alcohol consumption above 16 g per day (group 3 and 4 combined) resulted in a significant reduction in mortality from CHD (RR=0.14; 95% CI: 0.02 to 1.04; p=0.024). Moderate alcohol consumption (16 to 30 g per day) also reduced deaths from all causes (RR=0.36; 95% CI: 0.09 to 0.99; p=0.047). Low (p=0.491) and high (p=0.204) alcohol intake did not significantly impact on mortality in this population. Subanalyses using the Cox proportional hazard model and adjusted for age, duration of diabetes, BMI, cholesterol level, systolic blood pressure and smoking (Tables 2 and 3) indicated a significant reduction (p=0.023) in relative risk of all-cause mortality in men with light to moderate alcohol consumption (0 to 30 g per day). No such effect of alcohol consumption on mortality was shown in women (p=0.598). Similar analyses on the risk of death from CHD are not included, as they would be based primarily on only five events in people with light or moderate alcohol consumption (1 to 30 g per day).
Discussion
Prospective epidemiological studies have shown that moderate alcohol consumption noticeably reduces the risk of cardiovascular morbidity and mortality [3, 4, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26]. These studies primarily targeted healthy adults and showed that moderate alcohol consumption led to a 20 to 60% reduction of cardiovascular mortality. Recent data obtained in North American populations also suggest that moderate alcohol consumption has a beneficial effect on cardiovascular morbidity [27] and mortality [7, 8, 9, 10] in patients with Type 2 diabetes. However, the two recently published reports had a shorter follow-up than our study and included health professionals, who are in many respects specific study populations [8, 10]. One study had a comparable mixed population and similar follow-up to ours [7], but it investigated people with a mean age of 68 years, a large proportion (50%) of whom were being treated with insulin. In contrast, our study had younger patients (mean age 46 years), and fewer patients dependent on insulin. This could partly explain why CHD-related deaths occurred in only about 10% of our study population, compared to 20% in the study referred to [7]. Moreover, 53% of people in our study did not drink, whereas 10% were ranked as heavy drinkers (more than 30 g alcohol per day). In the US study [7] only 43% were non-drinkers and less than 4% were heavy drinkers. Despite these differences, the relative risk of death from CHD was reduced to a similar extent in diabetic patients in Europe and the United States [7] with moderate alcohol consumption, indicating that ethnicity, drinking pattern and type of alcoholic beverage have little effect on the protective effects of alcohol consumption. Similar findings on selected populations (US male physicians and US female nurses [8, 10]) and a recent study on drinking pattern and type of beverages [11] support this hypothesis.
When adjusted for other cardiovascular risk factors, the cardioprotective effect of moderate alcohol consumption remained in Type 2 diabetic men. In the Type 2 diabetic women of our cohort no significant cardioprotective effect could be shown. This contrasts to previous findings in a healthy population [4] and in diabetic women [8]. The most likely reason for this discrepancy is that the majority of women in our study were non-drinkers (79.2%) or consumed a maximum of 15 g alcohol per day (12%). Only 8.8% of the diabetic women consumed 16 g or more alcohol per day. The limited number of patients included in the study and the moderate alcohol consumption by a small number of women did not allow us to detect an effect on mortality in women.
In contrast to previous reports, our study also investigated the relative risk of all-cause mortality in association with alcohol consumption, providing evidence that moderate alcohol consumption has a beneficial effect on CHD mortality, while also reducing all-cause mortality. Our data do not explain these findings. They do, however, indicate that moderate alcohol intake (16 to 30 g per day) was beneficial with regard to mortality from CHD and from all causes, whereas lower and higher alcohol consumption were associated with a tendency towards a higher mortality risk. This suggests that the relationship between alcohol consumption and mortality is depicted by a U-shaped curve, which is consistent with several epidemiological studies on the relationship between alcohol consumption and all-cause mortality [2, 5] or cardiovascular disease [28, 29]. The underlying mechanisms for this U-shaped curve are ill defined. However, most of the studies claim that the descending limb of the curve is attributable to reduced death from cardiovascular disease [28, 30]. High alcohol consumption facilitates the progression of neuropathy [31] and suppresses hepatic gluconeogenesis, thus increasing the risk of hypoglycaemia [32]. It is not clear whether these factors contribute to the greater mortality observed with high alcohol consumption or whether other confounding factors, e.g. life-style associated with high alcohol intake, contribute to the present and previous findings.
The power of our study lies in its well-defined cohort of European Type 2 diabetic patients (the Swiss cohort of a multinational WHO study), the long follow-up period and small dropout rate. We cannot exclude the possibility that our small sample size failed to allow detection of subtle differences in mortality rates, particularly in women. Moreover, it cannot be ruled out that the group with light to moderate alcohol intake contained especially healthy patients, with moderate alcohol consumption simply a marker of overall healthy behaviour, as suggested previously [10].
In summary, this study confirms that moderate alcohol consumption reduces CHD mortality as well as all-cause mortality in a relatively young, well-defined European diabetic cohort. Although the associations observed do not prove a causal relationship, our findings indicate that moderate intake of alcohol can be tolerated in the diet of patients with diabetes mellitus. However, in light of major clinical and public health problems associated with heavy drinking, recommendations on alcohol consumption must be made on an individual basis, after carefully assessing the risks and benefits of changes in drinking behaviour.
Abbreviations
- HR:
-
Hazard ratio
- ICD-9:
-
International Classification of Disease 9
- RR:
-
risk rate
References
Klatsky AL, Armstrong MA, Friedman GD (1992) Alcohol and mortality. Ann Intern Med 117:646–654
Gronbaek M, Deis A, Sorensen TI et al. (1994) Influence of sex, age, body mass index, and smoking on alcohol intake and mortality. BMJ 308:302–306
Doll R, Peto R, Hall E, Wheatley K, Gray R (1994) Mortality in relation to consumption of alcohol: 13 years' observations on male British doctors. BMJ 309:911–918
Fuchs CS, Stampfer MJ, Colditz GA et al. (1995) Alcohol consumption and mortality among women. N Engl J Med 332:1245–1250
Marmot MG, Rose G, Shipley MJ, Thomas BJ (1981) Alcohol and mortality: a U-shaped curve. Lancet 1:580–583
Thun MJ, Peto R, Lopez AD et al. (1997) Alcohol consumption and mortality among middle-aged and elderly U.S. adults. N Engl J Med 337:1705–1714
Valmadrid CT, Klein R, Moss SE, Klein BE, Cruickshanks KJ (1999) Alcohol intake and the risk of coronary heart disease mortality in persons with older-onset diabetes mellitus. JAMA 282:239–246
Solomon CG, Hu FB, Stampfer MJ et al. (2000) Moderate alcohol consumption and risk of coronary heart disease among women with type 2 diabetes mellitus. Circulation 102:494–499
Tanasescu M, Hu FB, Willett WC, Stampfer MJ, Rimm EB (2001) Alcohol consumption and risk of coronary heart disease among men with type 2 diabetes mellitus. J Am Coll Cardiol 38:1836–1842
Ajani UA, Gaziano JM, Lotufo PA et al. (2000) Alcohol consumption and risk of coronary heart disease by diabetes status. Circulation 102:500–505
Mukamal KJ, Conigrave KM, Mittleman MA et al. (2003) Roles of drinking pattern and type of alcohol consumed in coronary heart disease in men. N Engl J Med 348:109–118
Teuscher A, Herman JB, Studer PP (1983) [Vascular diseases in 534 Swiss diabetics within the scope of a multinational study]. Klin Wochenschr 61:139–149
Jarrett RJ, Keen H, Grabauskas V (1979) The WHO multinational study of vascular disease in diabetes: 1. General description. Diabetes Care 2:175–186
Anonymous (1985) Prevalence of small vessel and large vessel disease in diabetic patients from 14 centres. The World Health Organisation Multinational Study of Vascular Disease in Diabetics. Diabetes Drafting Group. Diabetologia 28 [Suppl]:615–640
Anonymous (1977) International Classification of Diseases, Ninth Revision (ICD-9). World Health Organization (WHO), Geneva
Klatsky AL, Armstrong MA, Friedman GD (1997) Red wine, white wine, liquor, beer, and risk for coronary artery disease hospitalization. Am J Cardiol 80:416–420
Maclure M (1993) Demonstration of deductive meta-analysis: ethanol intake and risk of myocardial infarction. Epidemiol Rev 15:328–351
Goldberg RJ, Burchfiel CM, Reed DM, Wergowske G, Chiu D (1994) A prospective study of the health effects of alcohol consumption in middle-aged and elderly men. The Honolulu Heart Program. Circulation 89:651–659
Hein HO, Suadicani P, Gyntelberg F (1996) Alcohol consumption, serum low density lipoprotein cholesterol concentration, and risk of ischaemic heart disease: six year follow up in the Copenhagen male study. BMJ 312:736–741
Camargo CA Jr, Hennekens CH, Gaziano JM, Glynn RJ, Manson JE, Stampfer MJ (1997) Prospective study of moderate alcohol consumption and mortality in US male physicians. Arch Intern Med 157:79–85
Camargo CA Jr, Stampfer MJ, Glynn RJ et al. (1997) Moderate alcohol consumption and risk for angina pectoris or myocardial infarction in U.S. male physicians. Ann Intern Med 126:372–375
Keil U, Chambless LE, Doring A, Filipiak B, Stieber J (1997) The relation of alcohol intake to coronary heart disease and all-cause mortality in a beer-drinking population. Epidemiology 8:150–156
Rehm JT, Bondy SJ, Sempos CT, Vuong CV (1997) Alcohol consumption and coronary heart disease morbidity and mortality. Am J Epidemiol 146:495–501
Wannamethee SG, Shaper AG (1997) Lifelong teetotallers, ex-drinkers and drinkers: mortality and the incidence of major coronary heart disease events in middle-aged British men. Int J Epidemiol 26:523–531
Kitamura A, Iso H, Sankai T et al. (1998) Alcohol intake and premature coronary heart disease in urban Japanese men. Am J Epidemiol 147:59–65
Renaud SC, Gueguen R, Schenker J, d'Houtaud A (1998) Alcohol and mortality in middle-aged men from eastern France. Epidemiology 9:184–188
Wakabayashi I, Kobaba-Wakabayashi R, Masuda H (2002) Relation of drinking alcohol to atherosclerotic risk in type 2 diabetes. Diabetes Care 25:1223–1228
Rimm EB, Williams P, Fosher K, Criqui M, Stampfer MJ (1999) Moderate alcohol intake and lower risk of coronary heart disease: meta-analysis of effects on lipids and haemostatic factors. BMJ 319:1523–1528
Stampfer MJ, Colditz GA, Willett WC, Speizer FE, Hennekens CH (1988) A prospective study of moderate alcohol consumption and the risk of coronary disease and stroke in women. N Engl J Med 319:267–273
Gronbaek M (1999) Type of alcohol and mortality from cardiovascular disease. Food Chem Toxicol 37:921–924
McCulloch DK, Campbell IW, Prescott RJ, Clarke BF (1980) Effect of alcohol intake on symptomatic peripheral neuropathy in diabetic men. Diabetes Care 3:245–247
Yki-Jarvinen H, Koivisto VA, Ylikahri R, Taskinen MR (1988) Acute effects of ethanol and acetate on glucose kinetics in normal subjects. Am J Physiol 254:E175–180
Acknowledgements
We are indebted to the 287 study participants their relatives, as well as their physicians and staff, for their participation, help and support throughout the study. We are also grateful for the support we received from the Federal Office of Statistics, Neuchatel, Switzerland (Dr T. Spuler) and from the various community-based population registries throughout the country. We thank E. Hurni, Dr P.P. Studer, Dr H. Schnell and K. Diem for help with data collection and verification, and Dr A. Troendle for suggestions regarding the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Diem, P., Deplazes, M., Fajfr, R. et al. Effects of alcohol consumption on mortality in patients with Type 2 diabetes mellitus. Diabetologia 46, 1581–1585 (2003). https://doi.org/10.1007/s00125-003-1209-2
Received:
Revised:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-003-1209-2