
Purpose: The main aim of our study was to find out whether the combined use of neuronavigation and intraoperative MRI can increase the rate of “complete tumor removal”. The second aim was to characterize the different forms of surgically induced enhancement in order to differentiate them from residual tumor.
Materials and methods: Surgery was performed in 18 patients with high-grade glioma. Using a neuronavigation device, the surgeons operated up to the point where they would otherwise have terminated surgery. Intraoperative MRI was then performed to determine whether residual enhancing had been left behind and to update the neuronavigation device. If necessary, feasible surgery was continued. On days 1–3 after surgery early postoperative MRI (1.5 T) was performed. The proportion of patients in whom the enhancing tumor was completely removed was compared with a series of 60 patients with glioblastoma multiforme, who had been operated on using neither neuronavigation nor intraoperative MRI . We also looked for and characterized different types of surgically induced enhancement.
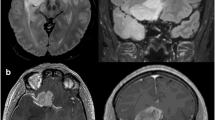
Results: Intraoperative MRI definitely showed residual tumor in 6 of the 18 patients and resulted in ambiguous findings in 3 patients. In 7 patients surgery was continued. Early postoperative MRI showed residual tumor in 3 patients and resulted in uncertain findings in 2 patients. The rate of patients in whom complete removal of enhancing tumor could be achieved was 50 % at the time of the intraoperative MR examination and 72 % at the time of the early postoperative MR control. The difference in proportion of patients with “complete tumor removal” between the groups who had been operated on using neuronavigation (NN) and intraoperative MRI (ioMRI) and those who had been operated on using only modern neurosurgical techniques except NN and ioMRI was statistically highly significant (Fisher exact test; P = 0.008). Four different types of surgically induced contrast enhancement were observed. These phenomena carry different confounding potentials with residual tumor.
Conclusion: Our preliminary experience with intraoperative MRI in patients with enhancing intraaxial tumors is encouraging. Combined use of neuronavigation and intraoperative MRI was able to increase the proportion of patients in whom complete removal of the enhancing parts of the tumor was achieved. Surgically induced enhancement requires careful analysis of the intraoperative MRI in order not to confuse it with residual tumor.
Zusammenfassung
Auch für erfahrene Neurochirurgen ist es außerordentlich schwierig bis unmöglich, intraoperativ die Grenze eines hirneigenen Tumors zu erkennen und entsprechend dieser Grenze eine „Totalentfernung“ des Tumors durchzuführen. Verschiedene Studien zeigten die Unzuverlässigkeit der intraoperativen Einschätzung der Operationsradikalität. Während intraoperative CT-Kontrollen und intraoperative Ultraschallkontrollen bereits seit längerem eingesetzt werden, wurde der Magnetresonanztomographie – der bildgebenden Methode mit der höchsten Weichteilauflösung – dieser Anwendungsbereich erst kürzlich durch die Entwicklung „offener“ MR-Systeme erschlossen. Im Operationstrakt der neurochirurgischen Klinik der Universität Heidelberg wurde ein offener MR-Tomograph installiert, an dem neben Biopsieentnahmen und neurochirurgischen Interventionen auch intraoperative MR-Kontrollen der Operationsradikalität durchgeführt werden. Unsere ersten Erfahrungen deuten darauf hin, daß durch den Einsatz intraoperativer MRT die Operationsradikalität neurochirurgischer Eingriffe gesteigert werden kann. Allerdings war bei allen Patienten durch die chirurgische Manipulation selbst verursachtes Kontrastmittelenhancement nachweisbar, das z. T. Verwechslungspotential mit Resttumor besaß.
Similar content being viewed by others


Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Knauth, M., Wirtz, C., Tronnier, V. et al. Intraoperative MRI to control the extent of brain tumor surgery. Radiologe 38, 218–224 (1998). https://doi.org/10.1007/s001170050345
Issue Date:
DOI: https://doi.org/10.1007/s001170050345