
Abstract
Purpose
Nonoperative management (NOM) of gunshot liver injuries (GLI) is infrequently practiced. The aim of this study was to assess the safety of selective NOM of GLI.
Methods
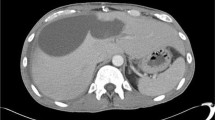
A prospective, protocol-driven study, which included patients with GLI admitted to a level 1 trauma center, was conducted over a 52-month period. Stable patients without peritonism or sustained hypotension with right-sided thoracoabdominal (RTA) and right upper quadrant (RUQ), penetrating wounds with or without localized RUQ tenderness, underwent contrasted abdominal CT scan to determine the trajectory and organ injury. Patients with established liver and/or kidney injuries, without the evidence of hollow viscus injury, were observed with serial clinical examinations. Outcome parameters included the need for delayed laparotomy, complications, the length of hospital stay and survival.
Results
During the study period, 54 (28.3%) patients of a cohort of 191 patients with GLI were selected for NOM of hemodynamic stability, the absence of peritonism and CT imaging. The average Revised Trauma Score (RTS) and Injury Severity Score (ISS) were 7.841 and 25 (range 4–50), respectively. 21 (39%) patients had simple (Grades I and II) and 33 (61%) patients sustained complex (Grades III to V) liver injuries. Accompanying injuries included 12 (22.2%) kidney, 43 (79.6%) diaphragm, 20 (37.0%) pulmonary contusion, 38 (70.4%) hemothoraces, and 24 (44.4%) rib fractures. Three patients required delayed laparotomy resulting in an overall success of NOM of 94.4%. Complications included: liver abscess (1), biliary fistula (5), intrahepatic A-V fistula (1) and hospital-acquired pneumonia (3). The overall median hospital stay was 6 (IQR 4–11) days, with no deaths.
Conclusion
The NOM of carefully selected patients with GLI is safe and associated with minimal morbidity.

Similar content being viewed by others

References
Navsaria PH, Berli J, Edu S, Nicol AJ. Non-operative management of abdominal stab wounds: an analysis of 186 patients. S Afr J Surg. 2007;45:128–32.
Moore EE. When is nonoperative management of a gunshot wound to the liver appropriate? J Am Coll Surg. 1999;188:427–8.
Garrett KA, Stain SC, Rosati C. Nonoperative management of liver gunshot injuries. Curr Surg. 2006;63:169–73.
Navsaria PH, Nicol AJ, Krige JE, Edu S. Selective nonoperative management of liver gunshot Injuries. Ann Surg. 2009;249:653–6.
Demetriades D, Rabinowitz B, Sofianos C. Non operative management of penetrating liver injuries: a prospective study. Br J Surg. 1986;73:736–7.
Scalea TM. Penetrating Liver Injuries. Curr Trauma Rep. 2015;1(2):69–75.
Renz BM, Feliciano DV. Gunshot wounds to the right thoracoabdomen: a prospective study of nonoperative management. J Trauma. 1994;37:737–44.
Chmielewski GW, Nicholas JM, Dulchavsky SA, Diebel LN. Nonoperative management of gunshot wounds of the abdomen. Am Surg. 1995;61:665–8.
Ginzburg E, Carrillo EH, Kopelman T, McKenney MG, Kirton OC, Shatz DV, et al. The role of computed tomography in selective management of gunshot wounds to the abdomen and flank. J Trauma. 1998;45:1005–9.
Demetriades D, Gomez H, Chahwan S, Charalambides K, Velmahos G, Murray J, et al. Gunshot injuries to the liver: the role of selective nonoperative management. J Am Coll Surg. 1999;188:343–8.
Omoshoro-Jones JA, Nicol AJ, Navsaria PH, Zellweger R, Krige JE, Kahn D. Selective non-operative management of liver gunshot injuries. Br J Surg. 2005;92:890–5.
Pal KM, Khan A. Nonoperative management of penetrating liver trauma. Injury. 2000;31:199–201.
Shanmuganathan K, Mirvis SE, Chiu WC, Killeen KL, Scalea TM. Triple-contrast helical CT in penetrating torso trauma: a prospective study to determine peritoneal violation and the need for laparotomy. Am J Roentgenol. 2001;177:1247–56.
DuBose J, Inaba K, Teixeira PG, Pepe A, Dunham MB, McKenney M. Selective nonoperative management of solid organ injury following abdominal gunshot wounds. Injury. 2007;38:1084–90.
Marr JDF, Krige JEJ, Terblanche J. Analysis of 153 gunshot wounds of the liver. Br J Surg. 2000;87:1030–4.
Demetriades D, Hadjizacharia P, Constantinou C, Brown C, Inaba K, Rhee P, et al. Selective nonoperative management of penetrating abdominal solid organ injuries. Ann Surg. 2006;244:620–8.
Renz BM, Bott J, Feliciano DV. Failure of nonoperative treatment of a gunshot wound to the liver predicted by computed tomography. J Trauma. 1996;40:191–93.
Dabbs DN, Stein DM, Scalea TM. Major hepatic necrosis: a common complication after angioembolization for treatment of high-grade liver injuries. J Trauma Acute Care Surg. 2009;66(3):621–9.
Michailidou M, Velmahos GC, Wilden G, Alam HB, de Moya M, Chang Y. Blush on trauma computed tomography: not as bad as we think. J Trauma Acute Care Surg. 2012;73(3):580–6.
Dabbs DN, Stein DM, Philosophe B, Scalea TM. Treatment of major hepatic venous: lobectomy versus serial debridements. J Trauma. 2010;69:562–67.
Philips T, Scalafini SJ, Goldstein A, Scalea T, Panetta T, Shaftan G. Use of contrast–enhanced CT enema in the management of penetrating trauma of the flank and back. J Trauma 986; 6:593–601.
Sherck J, Shatney C, Sensaki K, Selivanov V. The accuracy of computed tomography in the diagnosis of blunt small bowel perforation. Am J Surg. 1994;168:670–5.
Bala M, Gazalla SA, Faroja M, Bloom AI, Zamir G, Rivkind AI, et al. Complications of high grade liver injuries: management and outcome with focus on bile leaks. Scand J Trauma Resusc Emerg Med. 2012;20:20. https://doi.org/10.1186/1757-7241-20-20 (PMCID: PMC3352307).
Navsaria PH, Nicol AJ. Selective nonoperative management of kidney gunshot injuries. World J Surg. 2009;33:553–7.
Velmahos GC, Demetriades D, Cornwell EE III, et al. Selective management of renal gunshot wounds. Br J Surg. 1998;85:1121–4.
Wessells H, McAninch JW, Meyer A, Bruce J. Criteria for nonoperative management of significant penetrating renal lacerations. J Urol. 1997;157:2427.
Moolman C, Navsaria PH, Lazarus J, Pontin A, Nicol AJ. Nonoperative management of penetrating kidney injuries: a prospective audit. J Urol. 2012;188:169 – 73.
Leukhardt WH, Golob JF, McCoy AM, Fadlalla AM, et al. Follow-up disparities after trauma: a real problem for outcomes research. Am J Surg. 2010;199:348–53.
Funding
There is no funding source.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Drs. Pradeep Navsaria, Andrew Nicol, Jake Krige, Sorin Edu and Sharfuddin Chowdhury declare that they have no conflict of interest.
Ethical approval
The study has been approved by the institutional ethics committee and has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards: University of Cape Town Human Research Ethics Committee approved study: 048/2007.
Informed consent
This was a retrospective review of prospectively collected data (observational study); therefore, no consent was taken. The patients were managed according to standard Unit protocols. All data were collected by the first author on a password-protected computer and Excel sheet. None of the patients could be identified in the database as they were numbered consecutively from 1 to 278. The privacy and confidentiality interests of participants were preserved. No information can identify individuals.
Rights and permissions
About this article

Cite this article
Navsaria, P., Nicol, A., Krige, J. et al. Selective nonoperative management of liver gunshot injuries. Eur J Trauma Emerg Surg 45, 323–328 (2019). https://doi.org/10.1007/s00068-018-0913-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-018-0913-z