
Abstract
Purpose
The usefulness of chest wall stabilization after blunt chest wall trauma with unstable rib fractures has recently been intensely discussed. Thereby, the surgical approach seems to influence outcome, mortality and the long-term complication rate including chronic chest pain, thoracic deformity and quality of life. Here, we present the outcome after surgical stabilization of unstable rib fractures using intramedullary splints and plate osteosynthesis.
Methods
n = 50 patients were enrolled in this trial. Surgical stabilization was performed using intramedullary splints and/or plate osteosynthesis. Video-assisted thoracoscopy was performed in all patients for the inspection of the thoracic cavity and to exactly localize the fractured ribs. The pre- and postoperative pain course was documented using the visual analog scale.
Results
A total of n = 50 patients (10 females, mean age 63 years) were included into the analysis. All patients presented with traumatic serial rib fractures with a mean of 3 fractured ribs (range 2–8 ribs) and an unstable thorax wall. Rib osteosynthesis was performed using intramedullary splints (n = 17 patients), locking plates (n = 17 patients), or a combined use of both procedures (n = 16 patients). Mean operating time was 80 min (31–161 min). No major complications were seen intra- and postoperatively. Mean hospital stay was 8 ± 2 days (2–21 days). In all patients, excellent chest wall stability was achieved. Moreover, a significant reduction of pain was observed (2.6 ± 0.3 postoperatively vs. 8 ± 1.15 preoperatively, p < 0.0001) already during the hospital stay.
Conclusions
Rib osteosynthesis is a safe and effective treatment option for patients with unstable rib fractures after blunt chest wall trauma. It leads to a significant reduction of the trauma-associated pain caused by the rib fractures and supports a quick recovery of the patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Blunt chest wall trauma is associated with a high risk of morbidity and mortality [1,2,3]. Mostly, it is associated with unstable rib fractures (URF) leading to mechanical instability of the chest wall. URF could be accompanied by other injuries such as lung contusion, lung injury, hemothorax and pneumothorax. Additionally, it has been reported, that the incidence of pneumonia increases due to the number of fractured ribs especially in the elderly [4, 5]. Chronic pain and disability also may remain as long-term complications after chest wall injury and URF. Concerning those complications, several studies and reviews show that surgical approaches of chest wall stabilization in the scenario of a flail chest influence the outcome of patients. They decrease the pneumonia rate, positively affect chest deformity, tracheostomy rate, the duration of mechanical ventilation, the length of ICU stay and the overall hospital stay [6,7,8,9]. Hence, surgical stabilization of fractured ribs has become increasingly popular and the spectrum of the surgical techniques has increasingly applied less-invasive approaches [10].
The aim of this study was to assess the efficacy and postoperative outcome after rib osteosynthesis with intramedullary splints and/or plate osteosynthesis in the scenario of URF.
Patients and methods
Between 12/2013 and 12/2017, n = 50 patients (32 males/18 females) with unstable rib fractures due to blunt chest wall trauma were prospectively enrolled in this study and data prospectively recorded. The mean age was 63 years (range 30–98 years). Patients’ characteristics are summarized in Table 1. Patients with at least n = 2 dislocated rib fractures with concomitant hemothorax and/or pneumothorax were included in a prospective non-randomized fashion. The following factors served as exclusion criteria: n = 1 fractured rib, polytrauma patients and patients with other co-injuries. In all cases, the patients were haemodynamically stable and no major intrapericardial vessels were found. Figure 1 demonstrates our institutional blunt chest trauma management. Prior to surgery, all patients received a computed tomography of the chest (CT) with 3D-reconstruction of the chest wall (Fig. 2). After Evaluation, surgical rib stabilization was performed within 24 h after admission to the emergency room. For pain management, standard analgesia with opioids (Naloxon/Oxycodon) was administered during the postoperative course in all patients.

Institutional blunt chest trauma management

3D-chest-CT. Computed tomography of the chest (CT) with 3D-reconstruction of the chest wall demonstrating instable serial rib fracture with dislocated rib fragments lateral and dorsal
Rib osteosynthesis was performed using intramedullary splints (group 1), locking plates (group 2) or both osteosynthetic procedures (group 3). Type of osteosynthesis material was determined preoperatively, depending on the localization of the rib fractures. Patients with multiple-fragment rib fracture, distant fractures of the same rib, or with multiple fractures of the anterior or posterior cortex underwent rib stabilization using locking plates. Transversal rib fractures or slightly oblique fractures were stabilized with an intramedullary splint. To reduce friction and postoperative pain, subscapular rib fractions were primary stabilized using intramedullary splints.
All patients gave their written consent to the surgery pre-operatively. For pain assessment, the visual analogue scale (VAS) was performed pre- and postoperatively (day of hospital discharge). Postoperative pain was considered as the primary endpoint in all groups. The duration of surgery and hospital stay were considered secondary outcomes (Table 2).
Statistical analysis
Continuous variables were described using means, standard deviations, and ranges. Boxplots show the distribution of the continuous variables within the groups. Comparisons between postoperative parameters of all groups were performed using unpaired t tests. Test results were reported as mean difference between both procedures and the corresponding 95% confidence interval (CI). The limits of the 95% CI will be interpreted in the sense of an equivalence test. Equivalence margins were not prespecified. Superiority p values of the unpaired t tests will be reported for informational purpose.
Surgical technique
Surgical stabilization was performed using intramedullary splints and/or plate osteosynthesis (MatrixRib, Synthes®, Germany) using a minimally invasive approach. Intraoperatively, a single-port video-assisted thoracoscopy was performed at first in all patients for the inspection of the thoracic cavity determining the exact localization of dislocated rib fractures and for evacuation of an eventually existing hemothorax. Subsequently, in n = 15 patients a mini-thoracotomy was performed to evacuate a possibly accompanying thoracic wall hematoma and finally to achieve thoracic wall stabilization using either splints, locking plates or both osteosynthetic procedures.
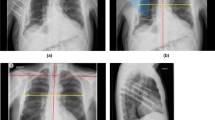
In all patients in group 1, a minimally invasive approach using an incision of 2 cm was performed to expose the area of the fracture. Subsequently, the splint was inserted under thoracoscopic visualization to confirm regular intramedullary positioning (Fig. 3).

Intraoperative images demonstrating the minimally invasive rib osteosynthesis using intramedullary splint. Through a single port VATS the affected ribs are localized (a). Thereafter, a 2 cm incision is made (d) to expose the area of the dislocated ribs (b). Subsequently, the intramedullary splints are inserted (b, c)
Results
Patients in this study presented with serial rib fractures of a mean of four ribs (range 2–8 ribs) with accompanying unstable chest wall. Among them, n = 7 patients were presented with two displaced fractured ribs. In these patients indication for surgery was the concomitant hemothorax (n = 5 patients) and persistent pneumothorax (n = 2 patients). Depending on the location of the fractures, rib osteosynthesis was achieved using intramedullary titanium splints in n = 17 patients, locking plates in n = 17 patients or both techniques in n = 16 patients. Thoracoscopic evacuation of a hemothorax due to rupture of the intercostal vessels was performed in n = 38 patients. In n = 8 patients, atypical wedge resection of injured lung tissue was performed. n = 10 patients presented with pneumothorax. In one case, a rupture of the diaphragm was sutured. n = 15 patients had significant soft tissue damage with pronounced hematoma.
Evaluating postoperative pain course, when analyzing all patients, a mean VAS of 2.6 ± 0.3 (range 1–5) postoperatively compared to a mean VAS of 8 ± 1.15 (range 5–10) preoperatively was documented (Fig. 4). Here, we could show a significant reduction of the pain already during the hospital stay (p < 0.0001, 95% CI − 5.68 to − 4.672). A comparison of techniques (groups) revealed no significant difference between group 1 (VAS of 2.6 ± 0.3, range 1–5) and group 2 (VAS of 3 ± 0.3, range 1–5) regarding postoperative pain course (p = 0.5, 95% CI − 0.58 to 1.18) (Fig. 3). The mean postoperative VAS in group 3 was 2.6 ± 0.3 (1–4). In addition, there were no significant differences in postoperative pain comparing group 1 vs. group 3 (p = 0.7, 95% CI − 0.92 to 0.62) and group 2 vs. group 3 (p = 0.3, 95% CI − 1.3 to 0.4). However, in all groups a significant reduction in pain could be seen after the procedure compared with preoperative levels, indicating that pain reduction is independent from the applied technique (Fig. 4).

Pain assessment. Pain assessment using the VAS shows a significant reduction in pain postoperatively in all patients. Comparing the postoperative pain course between the different groups no significant difference was noticed
The mean duration of surgery was 82 ± 5.4 min (range 31–215) in all groups. The mean duration of surgery was 61 ± 7.2 min (range 31–150) in group 1 and 94 ± 10.4 min (range 55–215) in group 2 (p = 0.01, 95% CI 6.55–58.6). Therefore, a significantly shorter duration of surgery was observed in group 1 compared with group 2 (Fig. 5). Comparing the duration of surgery between group 1 and group 3 (95 ± 8.1 min, range 42–161 min), operating time in group 1 was significantly shorter (p = 0.004, 95% CI 11.5–55.6). There was no difference in operating time seen between group 2 and 3 (p = 0.94, 95% CI − 26.5 to 28.41).

Duration of surgery. Data showed a significant reduction of the operating time for patients who only received intramedullary splints (group 1) compared to group 2 and group 3
The mean postoperative hospital stay was 8 ± 2 days (2–21 days) in all patients. The mean postoperative hospital stay was 6 ± 1 day (range 2–16) in group 1 compared to 9 ± 1 days (range 3–17) in group 2 (p = 0.07, 95% CI − 0.2 to 5.3), and to 10 ± 2 days (range 2–21) in group 3 (p = 0.05, 95% CI − 0.05 to 6.8). Although a clear trend toward shorter postoperative hospital stay was observed in group 1, no significance could be shown (Fig. 6). Comparing the postoperative hospital stay between group 2 and group 3, there was no statistical difference shown (p = 0.65, 95% CI − 2.97 to 4.63).

Postoperative hospital stay. Shows that the performed procedure did not have any influence on postoperative hospital stay. Although a clear trend toward shorter postoperative hospital stay was observed in group 1, no significance could be shown
No relevant complications were observed during the intra- and postoperative course. In all patients, excellent chest wall stability was achieved. Even at further follow-up at a mean of 16 ± 3 months (range 2–27) we did not notice any dislocation of the applied osteosynthesis and any instability.
Discussion
Blunt chest trauma is often associated with instable rib fractures, especially in elderly patients with the evidence of osteoporosis. This in particular influences mortality and morbidity. It affects appropriate breathing and ventilation leading to pneumonia in up to 30% of patients [1, 11].
The reasons for surgical rib fixation are the reduction of trauma-associated acute and chronic pain, optimization of the breathing excursion and ventilation and avoidance of mechanical ventilation. Although the surgical chest wall stabilization has become increasingly popular, especially in patients with a flail chest, the surgical approach remains controversial [12, 13].
Several surgical approaches for rib fixation have been described in the literature [10]. First, Jones and co-workers reported surgical rib fixation in 1926 in a patient with flail chest using a clamp which was fixed in the sternum and held under traction [14]. The high mortality rate associated with chest wall trauma, mostly as a complication of mechanical ventilation leading to pneumonia, induced intense activity in the development of novel surgical techniques and materials [15]. Dor et al. reported the first open surgical rib fixation using K-wires [16]. Other techniques applied intramedullary approaches, as well as suturing and bridging techniques, where fractured ribs were stabilized with metal wires and sutures. Due to insufficient results and a relevant number of reported complications, rib osteosynthesis using titanium plates has become more preferable [10].
Recent reports have demonstrated an association of minimally invasive surgical stabilization of a flail chest with reduced need for mechanical ventilation and a lower incidence of pneumonia [17, 18]. Bottlang et al. described the application of plates and intramedullary splints with promising results in a prospective study with 20 patients who underwent stabilization of a flail chest injury. Thereby, intramedullary rib splints provided a less-invasive and reliable fixation of rib fractures [19]. In a retrospective descriptive review of a clinical case series, Marasco et al. reported comparable results regarding functional recovery in patients after rib splinting compared to patients after plate osteosynthesis [20]. In our study, the use of splints, plates and the combination of both techniques were applied without any complications, achieving an excellent stabilization of the chest wall, leading to significant initial pain reduction. Additionally, in group comparison, no differences in postoperative pain course were documented.
Several randomized controlled trials have been published through the past decades comparing surgical approaches in the management of flail chest with conservative treatment. All these works demonstrated significant improvement after surgical stabilization with regards to the length of mechanical ventilation und ICU stay, as well as decreasing rate of pneumonia. Also a significant improvement in long-term outcome such as chest pain, chest tightness, dyspnea, time to return to work and ability to high-activity work was reported in several studies [4, 18, 21]. In contrast, Farquhar et al. reported recently a retrospective study including 19 patients that underwent surgical rib fixation and 36 patients with conservative management, that showed no benefit of surgical rib fixation vs. conservative treatment regarding time of mechanical ventilation, length of hospital stay and pneumonia onset. A limitation of this study was the small number of patients, especially in the surgical group. Furthermore, patients were considered for surgical rib fixation after ineffective conservative treatment. This could lead to selection bias and better results in the non-operative group. Therefore, an earlier surgical approach might lead to a better outcome in the surgical group [12]. In a retrospective study, DeFreest et al. reported longer hospitalization and ventilator duration for polytrauma patients after surgical rib fixation (n = 41 patients) compared to non-operative management (n = 45 patients). Limitations of this study were the heterogeneity of the polytrauma patients with different co-morbidities and co-injuries and the small number of patients involved. Furthermore, some of the patients in the surgical group were offered surgery several days after admission to the hospital. Although longer hospitalization in the surgical group was observed, mortality rate was lower compared to the non-operative group (n = 1 vs. n = 5 patients) [22].
In our study, 50 patients with blunt chest trauma and unstable rib fractures were subjected to rib osteosynthesis using plate osteosynthesis, intramedullary splinting and the combination of both techniques. After Evaluation, surgical rib stabilization was performed within 24 h after admission to the emergency room. Even in the postoperative course during the hospital stay, a significant reduction of pain was observed regardless the technique used. No postoperative mechanical ventilation was needed. Chest wall stability was achieved in all patients without any implant dislocation also at further follow up. Also no postoperative pneumonia developed in study patients. Therefore, early rib stabilization of the dislocated rib fractures and the instable chest wall is recommended in the early phase after blunt chest trauma, to prevent further complications.
The role of VATS in management of chest trauma has been described in the literature. In a small case series of hemodynamically stable patients with penetrating thoracic trauma and major lung or intercostal injuries without major intrapericardial vessels bleeding, VATS was successfully performed demonstrating the efficacy in acute trauma management [23]. Furthermore Jin et al. also demonstrated the efficacy of VATS for treatment of stable thoracic trauma patients compared to open thoracotomy in a randomized fashion [24]. Although a very sparse amount of randomized prospective data for the role of VATS in operative management of chest trauma patients exists, VATS can be beneficial in non-critical, hemodynamic stable patients. VATS can be a useful explorative and therapeutic procedure for non-major-vessel-bleeding hemothorax, pleural space debridement, lung parenchymal and diaphragmatic lesions [25, 26]. Therefore, thoracoscopic evaluation of the thoracic cavity can identify misdiagnosed lesions and avoid delayed complications.
Regarding the surgical approach, in our opinion, the minimally invasive technique for surgical rib fixation using intramedullary splints is a safe treatment option for patients with dislocated rib fractures after chest trauma. In comparison to conventional locking plates, they can be implanted minimally invasively using a significant shorter operating time. In multiple fractured ribs, locking plates seem to be the technique of choice but necessitate more invasive surgical incision.
Conclusion
Early rib osteosynthesis in patients with unstable rib fractures leads to a significant reduction of trauma associated pain. Rib fixation using intramedullary splints, locking plates or the combination of both operative techniques is a safe treatment option for patients after blunt chest trauma with dislocated rib fractures and an instable chest wall. Post-traumatic complications such as pneumonia, chest wall deformity and chronic pain are rare. The surgical stabilization reduces the pain by restoring the chest wall stability, which supports a quick recovery. It should be considered in the acute phase after chest traumatization and not only after failure of conservative treatment, where nociceptional mechanisms of chronic pain development have already been initiated.
References
Bulger EM, Arneson MA, Mock CN, Jurkovich GJ. Rib fractures in the elderly. J Trauma Injury Infect Crit Care. 2000;48(6):1040–6.
Ciraulo DL, Elliott D, Mitchell KA, Rodriguez A. Flail chest as a marker for significant injuries. J Am Coll Surg. 1994;178(5):466–70.
Lafferty PM, Anavian J, Will RE, Cole PA. Operative treatment of chest wall injuries: indications, technique, outcome. J Bone Joint Surg Am. 2011;93:97–110.
Tanaka H, Yukioka T, Yamaguti Y, Shimizu S, Goto H, Matsuda H, et al. Surgical stabilization of internal pneumatic stabilization? A prospective randomized study of management of severe flail chest patients. J Trauma. 2002;52(4):727–32.
Park HO, Kang DH, Moon SH, Yang JH, Kim SH, Byun JH. Risk factors for pneumonia in ventilated trauma patients with multiple rib fractures. Korean J Thorac Cardiovasc Surg. 2017;50:346–54.
Schuurmans J, Goslings JC, Schepers T. Operative management versus non-operative management of rib fractures in flail chest injuries: a systematic review. Eur J Trauma Emerg Surg. 2017;43:163–8.
Cataneo AJM, Cataneo DC, de Oliveira FHS, Arruda KA, El Dib R, de Oliveira Carvalho PE. Surgical versus nonsurgical interventions for flail chest. Cochrane Database Syst Rev. 2015;7:CD009919.
Slobogean GP, MacPherson CA, Sun T, Pelletier ME, Hameed SM. Surgical fixation vs. nonoperative management of flail chest: a meta-analysis. J Am Coll Surg. 2013;216:302–11.
Athanassiadi K, Gerazounis M, Theakos N. Management of 150 flail chest injuries: analysis of risk factors affecting outcome. Eur J Cardiothorac Surg. 2004;26:373–6.
Bemelman M, Poeze M, Blokhuis TJ, Leenen LP. Historic overview of treatment techniques for rib fractures and flail chest. Eur J Trauma Emerg Surg. 2010;36:407–15.
Sirmali M, Turut H, Topcu S, et al. A comprehensive analysis of traumatic rib fractures: morbidity, mortality and management. Eur J Cardiothorac Surg. 2003;24:133–8.
Farquhar J, Almahrabi Y, Slobogean G, et al. No benefit to surgical fixation of flail chest injuries compared with modern comprehensive management: results of a retrospective cohort study. Can J Surg. 2016;59(5):299–303.
De Jong MB, Kokke MC, Hietbrink F, Leenen LP. Surgical management of rib fractures: strategies and literature review. Scand J Surg. 2014;103:120–5.
Jones TB, Richardson EP. Traction on the sternum in the treatment of multiple fractured ribs. Surg Gynecol Obstet. 1926;42:283–5.
Relihan M, Litwin MS. Morbidity and mortality associated with flail chest injury: a review of 85 cases. J Trauma. 1973;13:663–71.
Dor V, Paoli JM, Noirclerc M, Malmejac C, Chauvin G, Pons R. Osteosynthesis of the thoracic wall: technic, results and indications: apropos of 19 cases. Ann Chir. 1967;21:983–96.
Doben AR, Eriksson EA, Denlinger CE, Leon SM, Couillard DJ, Fakhry SM, et al. Surgical rib fixation for flail chest deformity improves liberation from mechanical ventilation. J Crit Care. 2014;29:139–43.
Granetzny A, Abd El-Aal M, Emam E, Shalaby A, Boseila A. Surgical versus conservative treatment of flail chest. Evaluation of the pulmonary status. Interact Cardiovasc Thorac Surg. 2005;4:583–7.
Bottlang M, Long WB, Phelan D, Fielder D, Madey SM. Surgical stabilization of flail chest injuries with MatrixRIB implants: a prospective observational study. Injury. 2013;44(2):232–8.
Marasco S, Quayle M, Summerhayes R, Šutalo ID, Liovic P. An assessment of outcomes with intramedullary fixation of fractured ribs. J Cardiothorac Surg. 2016;11:126.
Marasco SF, Davies AR, Cooper J, Varma D, Bennett V, Nevill R, et al. Prospective randomized controlled trial of operative rib fixation in traumatic flail chest. J Am Coll Surg. 2013;216:924–32.
DeFreest L, Tafen M, Bhakta A, Ata A, Martone S, Glotzer O, Krautsak K, Rosati C, et al. Open reduction and internal fixation of rib fractures in polytrauma patients with flail chest. AMJ Surg. 2016;211:761–7.
Yu PS, Chan HH, Lau RW, Capili FG, Underwood MJ, Wan IY. Penetrating thoracic injury with retained foreign body: can video-assisted thoracic surgery take up the leading role in acute management? J Thorac Dis. 2016;8(8):2247–51.
Jin J, Song B, Lei YC, Leng XF. Video-assisted thoracoscopic surgery for penetrating thoracic trauma. Chin J Traumatol. 2015;18(1):39–40.
Chou YP, Lin HL, Wu TC. Video-assisted thoracoscopic surgery for retained hemothorax in blunt chest trauma. Curr Opin Pulm Med. 2015;21(4):393–8.
Mizobuchi T, Iwai N, Kohno H, Okada N, Yoshioka T, Ebana H. Delayed diagnosis of traumatic diaphragmatic rupture. Gen Thorac Cardiovasc Surg. 2009;57(8):430–2.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Akil, A., Ziegeler, S., Reichelt, J. et al. Rib osteosynthesis is a safe and effective treatment and leads to a significant reduction of trauma associated pain. Eur J Trauma Emerg Surg 45, 623–630 (2019). https://doi.org/10.1007/s00068-018-01062-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-018-01062-5