
Abstract
Purpose
Although they are considered the ‘gold standard’ of evidence-based medicine, randomized controlled trials are still a rarity in orthopedic surgery. In the management of patients with multiple trauma, there is a current trend toward ‘damage control orthopedics’, but to date, there is no proof of the superiority of this concept in terms of evidence-based medicine. The purpose of this article is to present unexpected difficulties we encountered in successfully completing our randomized controlled trial and to discuss the problematic differences between theoretically planning a trial and real-life practical experience of implementing the plan, with attention to published strategies.
Methods
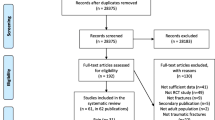
The multicenter randomized controlled trial on risk adapted damage control orthopedic surgery of femur shaft fractures in multiple trauma patients (DCO study) was designed to determine whether ‘risk adapted damage control orthopedics’ of femoral shaft fractures is advantageous when treating multiple trauma patients. We compared our methods of study planning and realization point by point with published methods for conducting such trials.
Results
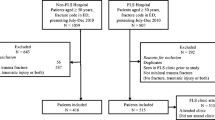
The study was methodically planned. We met the most prerequisites for successfully completing a large fracture trial, but experienced unexpected difficulties. After 2.5 years, the Deutsche Forschungsgemeinschaft suspended the financing because of low recruitment. The reasons were multifactorial.
Conclusions
We believe it is much more difficult to perform a large fracture trial in reality than to plan it in theory. Even the theoretically best designed trial can prove unsuccessful in its implementation. The question remains: are large fracture trials even possible? Hopefully YES!
Trial registration
Current Controlled Trials ISRCTN10321620. Date assigned: 09/02/2007.
Level of evidence
Level I.



Similar content being viewed by others

References
Trauma Registry of the German Trauma Society: annual reports. 2017. http://www.traumaregister.de.
Morshed S, Bhandari M. Clinical trial design in fracture-healing research: Meeting the challenge. J Bone Jt Surg Am. 2008;90(Suppl 1):55–61.
Bono CM, Tornetta P. Common errors in the desgin of orthopaedic studies. Injury. 2006;37:355–60.
Bhandari M, Pape HC, Giannoudis PV. Issues in the planning and conduct of randomised trials. Injury. 2006;37:349–54.
Simunovic N, Devereaux PJ, Bhandari M. Design considerations for randomised trials in orthopaedic fracture surgery. Injury. 2008;39:696–704.
Mejaddam AY, Velmahos GC. Randomized controlled trials affecting polytrauma care. Eur J Trauma Emerg Surg. 2012;38:211–21.
Hauser CJ, Boffard K, Dutton R, et al. Results of the CONTROL trial: efficacy and safety of recombinant activated Factor VII in the management of refractory traumatic hemorrhage. J Trauma. 2010;69:489–500.
Bartl C, Stengel D, Bruckner T, et al. Open reduction and internal fixation versus casting for highly comminuted and intra-articular fractures of the distal radius (ORCHID): protocol for a randomized clinical multi-center trial. Trials. 2011;22;12:84.
Rixen D, Steinhausen E, Sauerland S, et al. Protocol for a randomized controlled trial on risk adapted damage control orthopedic surgery of femur shaft fractures in multiple trauma patients. Trials. 2009;19;10:72.
Dutton R, Hauser C, Boffard K, et al. Scientific and logistical challenges in designing the CONTROL trial: recombinant factor VII in severe trauma patients with refractory bleeding. Clin Trials. 2009;6:467–79.
Rixen D, Grass G, Sauerland S, et al. Evaluation of criteria for temporary external fixation in risk-adapted damage control orthopedic surgery of femur shaft fractures in multiple trauma patients: “evidence-based medicine” versus “reality” in the trauma registry of the German Trauma Society. J Trauma. 2005;59:1375–94.
Rixen D, Steinhausen E, Sauerland S, et al. Randomized, controlled, two-arm, interventional, multicenter study on risk-adapted damage control orthopedic surgery of femur shaft fractures in multiple-trauma patients. Trials. 2016;25:17:47.
Csimma C, Swiontkowski MF. Large clinical trials in musculoskeletal trauma: Are they possible? J Bone Jt Surg. 2005;87:218–22.
Chan S, Bhandari M. The quality of reporting of orthopaedic randomized trials with use of a checklist for nonpharmacological therapies. J Bone Jt Surg Am. 2007;89:1970–8.
Jeray KJ, Tanner S, Schemitsch EH, et al. Are large fracture trials possible? J Orthop Trauma. 2010;24:S87–92.
MacKenzie EJ, Bosse MJ, Pollak AN, et al. Long-term persistence of disability following severe lower-limb trauma. Results of a seven-year follow-up. J Bone Jt Surg Am. 2005;87:1801–9.
Bhandari M, Guyatt G, Investigators, et al. Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures: Study to prospectively evaluate reamed intramedullary nails in patients with tibial fractures. J Bone Jt Surg Am. 2008;90:2567–78.
Helfet DL, Suk M, Hanson B. A critical appraisal of the SPRINT trial. Orthop Clin N Am. 2010;41:241–7.
Govender S, Csimma C, Genant HK, et al. Recombinant human bone morphogenetic protein-2 for treatment of open tibial fractures: a prospective, controlled, randomized study of four hundred and fifty patients. J Bone Jt Surg Am. 2002;84:2123–34.
Rixen D, Raum M, Bouillon B, et al. Predicting the outcome in severe injuries: an analysis of 2069 patients from the trauma register of the German Society of Traumatology (DGU). Unfallchirurg. 2001;104:230–9.
Dunham CM, Bosse MJ, Clancy TV, et al. Practice management guidelines for the optimal timing of long-bone fracture stabilization in polytrauma patients: the EAST Practice Management Work Group. J Trauma. 2001; 50:958–67.
Pape HC, Rixen D, Morley J, et al. Impact of the method of initial stabilization for femoral shaft fractures in patients with multiple injuries at risk for complications (borderline patients). Ann Surg. 2007;246:491–501.
Ferreira FL, Bota DP, Bross A, et al. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA. 2001;286:1754–8.
Morrison CA, Horwitz IB, Carrick MM. Ethical and legal issues in emergency research: barriers to conducting prospective randomized trials in an emergency setting. J Surg Res. 2009;157(1):115–22.
Rice TW, Morris S, Tortella BJ, et al. Deviations from evidence-based clinical management guidelines increase mortality in critically injured trauma patients. Crit Care Med. 2012;40(3):778–86.
Bednarska E, Bryant D, Devereaux PJ, et al. Orthopaedic surgeons prefer to participate in expertise-based randomized trials. Clin Orthop Relat Res. 2008;466:1734–44.
Soucacos PN, Johnson EO, Babis G. Randomised controlled trials in orthopaedic surgery and traumatology: Overview of parameters and pitfalls. Injury. 2008;39:636–42.
Bhandari M, Richards RR, Sprague S, et al. The quality of reporting of randomized trials in the Journal of Bone and Joint Surgery from 1988 through 2000. J Bone Jt Surg Am. 2002; 84A:388–96.
Huber-Wagner S, Lefering R, Qvick LM, et al. Effect of whole-body CT during trauma resuscitation on survival: a retrospective, multicentre study. Lancet. 2009;373:1455–61.
Brinck T, Handolin L, Paffrath T, et al. Trauma registry comparison: six-year results in trauma care in Southern Finland and Germany. Eur J Trauma Emerg Surg. 2015;41:509–16.
Timm A, Maegele M, Lefering R, et al. Pre-hospital rescue times and actions in severe trauma. A comparison between two trauma systems: Germany and the Netherlands. Injury. 2014;45(Suppl 3):S43–52.
Brinck T, Raj R, Skrifvars MB, et al. Unconscious trauma patients: outcome differences between Finland and Germany: lessons learned from trauma-registry comparisons. Eur J Trauma Emerg Surg. 2016;42:445–51.
Thien TM, Chatziagorou G, Garellick G, et al. Periprosthetic femoral fracture within two years after total hip replacement: analysis of 437,629 operations in the nordic arthroplasty register association database. J Bone Jt Surg Am. 2014;1;96(19):e167.
Cnudde PH, Kärrholm J, Rolfson O, et al. Cement-in-cement revision of the femoral stem: analysis of 1179 first-time revisions in the Swedish Hip Arthroplasty Register. Bone Jt J. 2017; 99-B(4 Supple B):27–32.
Acknowledgements
We are grateful to the members of the Study Steering Committee, the Data Safety Monitoring Board and the Ethics Committee for their supervision. We thank Dr. Melanie Affüpper-Fink (Institute for Research in Operative Medicine, University of Witten-Herdecke, Cologne, Germany), as well as the Coordinating Center for Clinical Studys Cologne (KKSK) for their help in performing the study.
Dr. G. Matthes1, PD Dr. H.J. Bail2, Dr. C. Grüber3, PD Dr. W. Zenker4, PD Dr. C. Burger5, Prof. Dr. D. Rixen6, Dr. E. Steinhauen6, Dr. G. Schiffer7, Prof. Dr. S. Flohe8, Dr. T. Lögters8, Prof. Dr. G. Täger9, Dr. B. Hußmann9, Prof. Dr. I. Marzi10, Dr. S. Wutzler10, Dr. A. Bonk11, Dr. M. Kremer11, Dr. L. Irlenbusch12, Prof. Dr. J.M. Rueger13, Prof. Dr. F. Hildebrand14, Dr. P. Mommsen14, Dr. O. Schoierer15, Dr. M. Burkhardt16, Dr. J. Scherer17, Prof. Dr. A. Seekamp18, Prof. Dr. C. Josten19, Dr. C. Wölfl20, Prof. Dr. C. Jürgens21, Dr. M. Zimmermann22, Prof. Dr. S. Ruchholtz23, Prof. Dr. W. Mutschler24, Dr. S. Huber-Wagner24, Dr. H. Trentzsch25, Dr. A. Ernstberger26, Prof. Dr. T. Mittlmeier27.
1Department of Trauma and Reconstructive Surgery, Unfallkrankenhaus Berlin (UKB), Berlin, Germany;2Center for Musculosceletal Surgery, Department of Trauma and Reconstructive Surgery, University of Berlin Charite Campus Virchow Clinic, Berlin, Germany;3Department of Trauma, Hand and Reconstructive Surgery, Helios Clinic Berlin-Buch, Berlin, Germany;4Department of Surgery, Trauma and Reconstructive Surgery Vivantes-Clinic Berlin, Berlin, Germany;5Department of Orthopedic and Trauma Surgery, University of Bonn, Bonn, Germany;6Department of Trauma Surgery, Orthopedics and Sporttraumatology, University of Witten-Herdecke at the Campus Cologne-Merheim, Cologne, Germany;7Department of Trauma, Hand and Reconstructive Surgery, University of Cologne, Cologne, Germany;8Department of Trauma and Hand Surgery, University of Düsseldorf, Düsseldorf, Germany;9Department of Trauma Surgery, University of Essen, Essen, Germany;10Department of Trauma, Hand and Reconstructive Surgery, Johann Wolfgang Goethe University Frankfurt, Frankfurt, Germany;11Center for Trauma Surgery, Berufsgenossenschaftliche Unfallklinik Frankfurt, Frankfurt, Germany;12Department of Trauma Surgery University of Halle, Halle, Germany;13Department of Trauma, Hand and Reconstructive Surgery, University of Hamburg, Hamburg, Germany;14Department of Trauma Surgery Medical University of Hannover, Hannover, Germany;15Department of Trauma Surgery, Surgical University Hospital Heidelberg, Heidelberg, Germany;16Department of Trauma, Hand and Reconstructive Surgery University of Saarland (Homburg), Homburg, Germany;17Department of Trauma Surgery, Clinic Ingolstadt, Ingolstadt, Germany;18Department of Trauma Surgery, University Hospitals Schleswig-Holstein, Campus Kiel, Kiel, Germany;19Department of Trauma and Reconstructive Surgery, University of Leipzig, Leipzig, Germany;20Department of Trauma Surgery, Berufsgenossenschaftliche Unfallklinik Ludwigshafen, Ludwigshafen, Germany;21Department of Trauma Surgery, University Hospitals Schleswig-Holstein, Campus Lübeck, Lübeck, Germany;22Department of Trauma Surgery, St. Marien-Hospital Lünen, Lünen, Germany;23Department of Trauma, Reconstructive and Hand Surgery, University of Marburg/Gießen, Marburg, Germany;24Department of Trauma Surgery, University of Munich, Campus Innenstadt, Munich, Germany;25Department of Trauma Surgery, University of Munich, Campus Großhadern, Munich, Germany;26Department of Trauma Surgery, University of Regensburg, Regensburg, Germany;27Department of Trauma and Reconstructive Surgery, University of Rostock, Rostock, Germany
Author information
Authors and Affiliations
Consortia
Contributions
ES: drafted the manuscript, was the study manager and coordinated multicenter management. BB: clinical scientific advisor and conceived and designed the study. DR: principal coordinating investigator, conceived and designed the study, and drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Funding
The Damage Control Study was funded by the Deutsche Forschungsgemeinschaft (grant number: RI 929/3-1).
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Steinhausen, E., Bouillon, B., Rixen, D. et al. Are large fracture trials really possible? What we have learned from the randomized controlled damage control study?. Eur J Trauma Emerg Surg 44, 917–925 (2018). https://doi.org/10.1007/s00068-017-0891-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-017-0891-6