
Abstract
Purpose
The aim of this study is to evaluate the early survival and organ damage following 30 and 60 min of thoracic resuscitative endovascular balloon occlusion of the aorta (REBOA) in an ovine model of severe hemorrhagic shock.
Methods
Eighteen sheep were induced into shock by undergoing a 35 % controlled exsanguination over 30 min. Animals were randomized into three groups: 60-min REBOA 30 min after the bleeding (60-REBOA), 30-min REBOA 60 min after the bleeding (30-REBOA) and no-REBOA control (n-REBOA). Resuscitation with crystalloids and whole blood was initiated 20 and 80 min after the induction of shock. Animals were observed for 24 h with serial potassium and lactate measurements. Autopsy was performed to evaluate organ damage.
Results
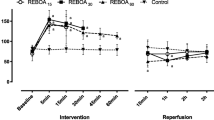
Two animals of the n-REBOA group died within 90 min of shock induction; no hemorrhagic deaths were observed in the REBOA groups. Twenty-four-hour survival for the 60-, 30-, and n-REBOA groups was 0/6, 5/6, and 4/6 (P = 0.002). In 60-REBOA, potassium and lactate were increased at 270-min time point: from 4.3 to 5.1 mEq/l and from 3.7 to 5.1 mmol/L, respectively. Both these values were significantly higher than in the n-REBOA group (P = 0.029 for potassium and P = 0.039 for lactate). Autopsy revealed acute tubular necrosis in all died REBOA group animals.
Conclusions
In this ovine model of severe hemorrhagic shock, REBOA can be used to prevent early death from hemorrhage; however, 60 min of occlusion results in significant metabolic derangement and organ damage that offsets this gain.



Similar content being viewed by others


References
Tien HC, Spencer F, Tremblay LN, et al. Preventable deaths from hemorrhage at a level I canadian trauma center. J Trauma. 2007;62(1):142–6.
Sanddal TL, Esposito TJ, Whitney JR, et al. Analysis of preventable trauma deaths and opportunities for trauma care improvement in Utah. J Trauma. 2011;70(4):970–7.
Seamon MJ, Haut ER, Van Arendonk K, et al. An evidence-based approach to patient selection for emergency department thoracotomy: A practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg. 2015;79(1):159–73.
Stannard A, Eliason JL, Rasmussen TE. Resuscitative endovascular balloon occlusion of the aorta (REBOA) as an adjunct for hemorrhagic shock. J Trauma. 2011;71(6):1869–72.
Moore LJ, Brenner M, Kozar RA, et al. Implementation of resuscitative endovascular balloon occlusion of the aorta as an alternative to resuscitative thoracotomy for noncompressible truncal hemorrhage. J Trauma Acute Care Surg. 2015;79(4):523–32.
Saito N, Matsumoto H, Yagi T, et al. Evaluation of the safety and feasibility of resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2015;78(5):897–904.
Carden DL, Granger DN. Pathophysiology of ischaemia-reperfusion injury. J Pathol. 2000;190(3):255–66.
Markov NP, Percival TJ, Morrison JJ, et al. Physiologic tolerance of descending thoracic aortic balloon occlusion in a swine model of hemorrhagic shock. Surgery. 2013;153(6):848–56.
Morrison JJ, Ross JD, Markov NP, et al. The inflammatory sequelae of aortic balloon occlusion in hemorrhagic shock. J Surg Res. 2014;191(2):423–31.
Abu-Nema T, Ayyash K, Berntman L, et al. Intraaortic balloon tamponade during hemorrhagic shock in sheep. Circ Shock. 1988;24(1):55–62.
Scott DJ, Eliason JL, Villamaria C, et al. A novel fluoroscopy-free, resuscitative endovascular aortic balloon occlusion system in a model of hemorrhagic shock. J Trauma Acute Care Surg. 2013;75(1):122–8.
Reva VA, Morrison JJ, Denisov AV, et al. Development of an ovine model of occlusive arterial injury for the evaluation of endovascular interventions. Vascular. 2015. doi:10.1177/1708538115615779.
Swindle MM, Smith AC. Comparative anatomy and physiology of the pig. Scand J Lab Anim Sci. 1998;25:11–21.
Martinelli T, Thony F, Decléty P, et al. Intra-aortic balloon occlusion to salvage patients with life-threatening hemorrhagic shocks from pelvic fractures. J Trauma. 2010;68:942–8.
Teeter WA, Matsumoto J, Idoguchi K, et al. Smaller introducer sheaths for REBOA may be associated with fewer complications. J Trauma Acute Care Surg. 2016. doi:10.1097/ta.0000000000001143.
Inoue J, Shiraishi A, Yoshiyuki A, et al. Resuscitative endovascular balloon occlusion of the aorta might be dangerous in patients with severe torso trauma: A propensity score analysis. J Trauma Acute Care Surg. 2016;80:559–67.
Brenner ML, Moore LJ, DuBose JJ, et al. A clinical series of resuscitative endovascular balloon occlusion of the aorta for hemorrhage control and resuscitation. J Trauma Acute Care Surg. 2013;75:506–11.
Horer TM, Cajander P, Anders J, et al. A case of partial aortic balloon occlusion in an unstable multi-trauma patient. Trauma. 2016;18(2):150–4.
Johnson MA, Neff LP, Williams TK, et al. Partial Resuscitative Balloon Occlusion of the AORTA (P-REBOA): Clinical Technique and Rationale. J Trauma Acute Care Surg. 2016. doi:10.1097/ta.0000000000001146.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Viktor Reva and Sergey Telickiy received a Grant from the President of Russia #MK-7508.2016.7 to conduct this study.
Conflict of interest
Yosuke Matsumura is a clinical advisory board member of Tokai Medical Products. Jonathan Morrison is a clinical advisory board member of Prytime Medical Inc. Tal Hörer, Denis Sveklov, Alexey Denisov, Alexey Seleznev, Elvira Bozhedomova, and Igor Samokhvalov declare that they have no conflict of interest.
Ethical approval
All procedures performed in this experimental study were in accordance with the ethical standards of the Kirov Military Medical Academy and National Institutes of Health guide for the care and use of laboratory animals. The local institutional ethics committee approved the study (protocol no. 163/2015).
Additional information
V. A. Reva and Y. Matsumura contributed equally to this paper.
Rights and permissions
About this article

Cite this article
Reva, V.A., Matsumura, Y., Hörer, T. et al. Resuscitative endovascular balloon occlusion of the aorta: what is the optimum occlusion time in an ovine model of hemorrhagic shock?. Eur J Trauma Emerg Surg 44, 511–518 (2018). https://doi.org/10.1007/s00068-016-0732-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-016-0732-z