
Abstract
Purpose
To assess the risk for technical complications in patients undergoing removal of locking compression plates (LCP) with head locking screws.
Methods
A total of 205 patients who were scheduled for implant removal surgery after a healed fracture of the femur, tibia, humerus, distal radius, or clavicle in nine Austrian clinics were prospectively included in the study, all of whom had previously undergone fracture fixation by plates, with titanium implants used in 98 % of the patients. Intraoperative technical complications and the methods used to solve them were documented by the surgeon.
Results
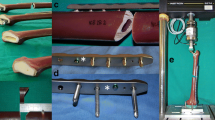
During the course of this study, a total of 1,462 locking screws were removed from 204 LCPs. While 95 % of these screws could be removed without difficulties, technical complications were reported for 41 patients with 78 screws which could not be removed with standard screwdrivers and required the use of additional instruments. The estimated risk for the occurrence of at least one technical complication during implant removal surgery was 20.1 %. The most frequently observed complications were screws that could not be loosened because they were jammed in the LCP, screws with a damaged recess in which the screwdriver turned freely, as well as a combination of both events. The majority of these screws could be removed with the use of a conical extraction screw or by drilling off the screw head. In one patient, an intraoperative refracture of the humerus occurred during plate removal. Even though there is a rate of 20 % for technical complications when removing the implants, only a few patients experience a clinical impact.
Conclusions
Titanium LCPs are prone to technical complications during implant removal, but the majority of the issues can be solved using special techniques.

Similar content being viewed by others


References
Ochs BG, Gonser CE, Baron HC, Stöckle U, Badke A, Stuby FM. Refracture of long bones after implant removal. An avoidable complication? Unfallchirurg. 2012;115:323–9.
Vos D, Hanson B, Verhofstad M. Implant removal of osteosynthesis: the Dutch practice. Results of a survey. J Trauma Manag Outcomes. 2012;6:6–13.
Hanson B, van der Werken C, Stengel D. Surgeons’ beliefs and perceptions about removal of orthopaedic implants. BMC Musculoskelet Disord. 2008;9:73–81.
Busam ML, Esther RJ, Obremskey WT. Hardware removal: indications and expectations. J Am Acad Orthop Surg. 2006;14:113–20.
Müller-Färber J. Removal of metal in traumatology. Unfallchirurg. 2003;106:653–68.
Wang J, Chidambaram R, Mok D. Is removal of clavicle plate after fracture union necessary? Int J Shoulder Surg. 2011;5:85–9.
Beaupre GS, Csongradi JJ. Refracture risk after plate removal in the forearm. J Orthop Trauma. 1996;10:87–92.
van Nortwick SS, Yao J, Ladd AL. Titanium integration with bone, welding, and screw head destruction complicating hardware removal of the distal radius: report of 2 cases. J Hand Surg Am. 2012;37:1388–92.
Hamilton P, Doig S, Williamson O. Technical difficulty of metal removal after LISS plating. Injury. 2004;35:626–8.
Suzuki T, Smith WR, Stahel PF, Morgan SJ, Baron AJ, Hak DJ. Technical problems and complications in the removal of the less invasive stabilization system. J Orthop Trauma. 2010;24:369–73.
Bae JH, Oh JK, Oh CW, Hur CR. Technical difficulties of removal of locking screw after locking compression plating. Arch Orthop Trauma Surg. 2009;129:91–5.
Ehlinger M, Adam P, Simon P, Bonnomet F. Technical difficulties in hardware removal in titanium compression plates with locking screws. Orthop Traumatol Surg Res. 2009;95:373–6.
Georgiadis GM, Gove NK, Smith AD, Rodway IP. Removal of the less invasive stabilization system. J Orthop Trauma. 2004;18:562–4.
Kumar G, Dunlop C. Case report: a technique to remove a jammed locking screw from a locking plate. Clin Orthop Relat Res. 2011;469:613–6.
Wagner M, Frigg R. AO manual of fracture management: internal fixators. Stuttgart: Thieme;2006. pp. 163–79.
Hayes JS, Seidenglanz U, Pearce AI, Pearce SG, Archer CW, Richards RG. Surface polishing positively influences ease of plate and screw removal. Eur Cell Mater. 2010;26:117–26.
Pearce AI, Pearce SG, Schwieger K, Milz S, Schneider E, Archer CW, Richards RG. Effect of surface topography on removal of cortical bone screws in a novel sheep model. J Orthop Res. 2008;26:1377–83.
Acknowledgments
The authors wish to thank the following Austrian investigators and clinics for their participation in documenting the patient data for this multicenter study: Alexander Auffarth, Trauma Clinic Medical University Salzburg; Michael Blauth, Christian Deml, Stefanie-Barbara Trulp, Luzian Haug, Department for Trauma Surgery, Medical University Innsbruck; Mark Passl, Patrick Bergthaler, Trauma Hospital Graz; Michael Wagner, Eva Fuchs, Wilhelminen Hospital Vienna; Stefan Hajdu, Constantin Dlaska, Trauma Clinic University Vienna; Alexander Meznik, Sonja El-Schahawi, Trauma Hospital Meidling Vienna; Benjamin Ramprecht, Trauma Hospital Klagenfurt.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schwarz, N., Euler, S., Schlittler, M. et al. Technical complications during removal of locking screws from locking compression plates: a prospective multicenter study. Eur J Trauma Emerg Surg 39, 339–344 (2013). https://doi.org/10.1007/s00068-013-0301-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-013-0301-7