
Abstract
Purpose
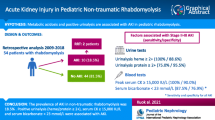
Rhabdomyolysis is a syndrome caused by musculoskeletal tissue damage that leads to the release of large amounts of intracellular elements, which particularly affect renal function. The most common causes are severe trauma, ischemia, surgical procedures, and drug abuse. We aimed to determine the incidence of rhabdomyolysis by measuring muscle injury markers (CK, myoglobin), to identify pre/post-admission as well as iatrogenic risk factors for rhabdomyolysis in severe polytrauma, to clarify the relevance of orthopedic injuries and surgical treatment in the onset/worsening of rhabdomyolysis, and to correlate risk factors with its main complication—acute renal failure (ARF).
Methods
Prospective study of severe polytrauma patients (Injury Severity Score (ISS) >15), with CK and myoglobin values measured at admission and after 24, 48, and 72 h. Peak values, variations between admission and peak, and variations between admission and day 3 were all determined. The correlations of those values with the onset of ARF and other negative outcomes were assessed.
Results
A total of 57 consecutive patients with a median ISS of 29 were included. ARF was present in 20 patients (38 %). CK-0 level was correlated with male gender (p < 0.027) and ISS (0.014); Mb-0 level was correlated with hypovolemic shock (0.003) and skeletal fracture (p < 0.043). CK-max was correlated with surgery (p < 0.038) and surgery duration (p < 0.014); Mb-max was correlated with surgery (p < 0.002) and anesthesia duration (p < 0.005). Δ-CK was correlated with surgery (p < 0.01) and surgery duration (p < 0.017), and Δ0-3-CK was correlated with surgery (p < 0.042). Logistic regression analysis found relationships between Δ0-3-CK and both ICU admission (p < 0.003) and MODS (p < 0.012), and between Mb-max and ARF (p < 0.034).
Conclusion
We found that a large number of factors are implicated in CK and Mb variations. Rhabdomyolysis is a very frequent complication, but increase in CK marker alone does not seem to be correlated with the incidence of ARF. Therefore, Mb level should be considered in this group of patients.



Similar content being viewed by others
References
Bywaters EGL, Beal D. Crush injuries with impairment of renal function. Br Med J. 1941;I:427–32.
Allison RC, Bedsole HL. The other medical causes of rhabdomyolysis. Am J Med Sci. 2003;326:79–88.
Graham DJ, Staffa JA, Shatin D, et al. Incidence of hospitalized rhabdomyolysis in patients with lipid lowering-drugs. LAMA. 2004;292:2585–90.
Richards JR. Rhabdomyolysis and drugs abuse. J Emerg Med. 2000;19:51–6.
Foster MR. Rhabdomyolysis in lumbar spine surgery: a case report. Spine. 2003;28:276–8.
Lim JK, Ang KC, Wang SC, Kumar VP. Rhabdomyolysis following shoulder arthroscopy. Arthtroscopy. 2006;22:1366e1–5.
Shing U, Scheld M. Infectious etiologies of rhabdomyolysis: three cases and a review. Clin Infect Dis. 1996;22:642–9.
Galvez R, Stacy J, Howley A. Exertional rhabdomyolysis in seven division-1 swimming athletes. Clin J Sports Med. 2008;18:366–8.
Mikkelsen TS, Toft P. The correlation between creatine kinase and myoglobin in critical ill patients with rhabdomyolysis. Crit Care Med. 2004;8:S155.
Lappalainen H, Tiula E, Uotila L. Elimination kinetics of myoglobin and creatine kinase. Crit Care Med. 2002;30:2212–5.
Vanholder R, Sever M, Erek E, Lameire N. Disease of the month: rhabdomyolysis. J Am Soc Nephrol. 2000;11:1153–61.
Criddle LM. Rhabdomyolysis: pathophysiology, recognition and management. Crit Care Nurse. 2003;23:14–30.
Sharp L, Rozycki G, Feliciano D. Rhabdomyolysis and secondary renal failure in critically ill surgical patients. Am J Surg. 2004;188:801–6.
Malinoski DJ, Slater MS, Mullins RJ. Crush injury and rhabdomyolysis. Crit Care Clin. 2004;20:171–92.
Gonzlez D. Crush syndrome. Crit Care Med. 2005;33:S34–41.
Brown CV, Rhee P, Evans K, Demetriades D, Velmahos G. Rhabdomyolysis after penetrating trauma. Am Surg. 2004;70:890–2.
Reis ND. Mechanical muscle-crush injury and acute muscle-crush compartment syndrome. J Bone Joint Surg (Br). 2005;87:450–3.
Better OS, Rubinstein I, Reis ND. Muscle crush compartment syndrome: fulminant local oedema with threatening systemic effects. Kid Int. 2003;63:1155–7.
Heppenstall RB, Scott R, Sapega A, Park YS, Chance B. A comparative study of the tolerance of skeletal muscle to ischaemia: tourniquet application compared eith acute compartment syndrome. J Bone Surg (Am). 1986;68:820–8.
Bagley WH, Yang H, Shah KH. Rhabdomyolysis. Intern Emerg Med. 2007;2:210–8.
Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, Levin A. Acute kidney injury network: report of an initiative to improve outcomes in acute kidney injury. Acute kidney injury network. Crit Care. 2007;11:R31.
Sheng Z-Y. Medical support in the Tangshan earthquake: a review of the management of mass casualties and certain major injuries. J Trauma. 1987;21:1130–4.
Kuwagata Y, Oda J, Tanaka H, et al. Analysis of 2702 traumatized patients in the 1995 Hanshin-Awaji earthquake. J Trauma. 1997;43:427–32.
Oda J, Tanaka H, Yoshioka T, et al. Analysis of 372 patients with crush syndrome caused by the Hanshin-Awaji earthquake. J Trauma. 1997;42:470–6.
Gunal AL, Celiker H, Dogukan A, et al. Early and vigorous fluid resuscitation prevents acute renal failure in the crush victims of catastrophic earthquakes. J Am Soc Nephrol. 2004;15:1862–7.
Brivet FG, Kleinknecht DJ, Loirat P, Landis PJM. Acute renal failure in intensive care units- causes, outcomes and prognostic factors of hospital mortality: a prospective multicenter study. Crit Care Med. 1996;24:192–8.
Slater MS, Mullins RJ. Rhabdomyolysis and myoglobinuric renal failure in trauma and surgical patients: a review. J Am Coll Surg. 1998;186:693–716.
Smith WA, Hardcastle TC. A crushing experience: the spectrum and outcome of soft tissue injury and myonephropathic syndrome at an urban south African University Hospital. Afr J Emerg Med. 2011;1:17–24.
Brown CV, Rhee P, Chan L, et al. Preventing renal failure in patients with rhabdomyolysis do bicarbonate and mannitol make a difference? J Trauma. 2004;56:1191–6.
Korthuis RJ, Granger DN, Townsley MI, Taylor AE. The role of oxygen-derived free radicals in ischemia-induced increases in canine muscle vascular permeability. Cir Res. 1985;57:599.
McCord JM. Oxygen derived free radicals in postischemia tissue injury. N Engl J Med. 1985;312:159–63.
Linas SL, Whittenberg D, Repine JE. Role of xanthenes oxidase in ischemia/reperfusion injury. Am J Physiol. 1990;258:F711–6.
Zager R. Mitochondrial free radical production induces lipid peroxidation during myohemoglobinuria. Kidney Int. 1996;49:741–51.
Lopez JR, Rojas B, Gonzalez MA, et al. Mycoplasmic Ca2+ concentration during exertional rhabdomyolysis. Lancet. 1995;345:424–5.
Harris AG, Skalat TC. Effects of leukocyte activation on capillary hemodynamics in skeletal muscle. Am J Physiol. 1993;264:H909–16.
Rehaman J, Boglia J, Chughtai B, Sukkarieh T, et al. High body mass index in muscular patients and flank position are risk factors for rhabdomyolysis: case report after laparoscopic live-donor nephrectomy. J Endourol. 2006;20:646–50.
Wakabayashi W, Kikuno T, Ohwada T, Kikawada R. Rapid fall in myoglobin in massive rhabdomyolysis and acute renal failure. Intensive Care Med. 1994;20:109–12.
Kumbhare D, Parkinson W, Dunlop B. Validity of serum creatine kinase as a measure of muscle injury produced by lumbar surgery. J Spinal Disord Tech. 2008;21:49–54.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sousa, A., Paiva, J.A., Fonseca, S. et al. Rhabdomyolysis: risk factors and incidence in polytrauma patients in the absence of major disasters. Eur J Trauma Emerg Surg 39, 131–137 (2013). https://doi.org/10.1007/s00068-012-0233-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-012-0233-7