
Abstract
Background and purpose
Patients with recurrent cervical cancer (RecCC) who received definitive radiochemotherapy including image-guided adaptive brachytherapy (IGABT) as primary treatment are currently treated in our institution with palliative intent by chemotherapy (CHT) combined with bevacizumab (BEV). We aim to evaluate the risk of gastrointestinal (GI)/genitourinary (GU) fistula formation in these patients.
Materials and methods
Data of 35 consecutive patients with RecCC treated initially with radiochemotherapy and IGABT were collected. Known and presumed risk factors associated with fistula formation were evaluated. Fistula rate was compared between patients receiving CHT or CHT+BEV.
Results
Of the 35 patients, 25 received CHT and 10 patients received CHT+BEV. Clinical characteristics were comparable. Fistulae were reported in 6 patients: two fistulae (8%) in the CHT group, four (40%) in the CHT+BEV group. GU fistula occurred in the CHT+BEV group only (3/4). Of these 6 patients with fistulae, 5 (83%) had undergone previous invasive procedures after the diagnosis of RecCC and 1 patient had undergone pelvic re-irradiation; 3/6 patients had developed a local recurrence. No other risk factors for fistula formation were identified.
Conclusion
In patients with RecCC after definitive radiochemotherapy including IGABT, the addition of BEV to CHT may increase the risk for GU fistula formation, particularly after invasive pelvic procedures. Future clinical studies are required to identify predictors for fistula formation to subsequently improve patient selection for the addition of BEV in the RecCC setting.
Zusammenfassung
Hintergrund und Ziel
Patientinnen mit Rezidiv eines Zervixkarzinoms (RecCC), die primär eine bildgesteuerte adaptive Brachytherapie (IGABT) und kombinierte Radiochemotherapie (RCHT) erhalten hatten, werden derzeit in unserem Institut mit einer Kombination aus Chemotherapie (CHT) und Bevacizumab (BEV) behandelt. Ziel dieser Studie war es, das Risiko für das Auftreten gastrointestinaler (GI) sowie urogenitaler (GU) Fisteln unter CHT sowie CHT + BEV zu analysieren.
Patienten und Methode
In diese retrospektive Datenanalyse wurden insgesamt 35 konsekutive Patientinnen mit RecCC, die primär mit RCHT und IGABT behandelt worden waren, inkludiert. Klinisch-pathologische Risikofaktoren für das Auftreten einer GI- sowie GU-Fistel wurden erhoben. Die Raten an Fistelbildungen in der CHT-Gruppe und in der Gruppe mit CHT + BEV wurden verglichen.
Ergebnisse
Von 35 Patientinnen erhielten 25 eine CHT und 10 CHT + BEV. Insgesamt wurde bei 6 Patientinnen eine Fistel diagnostiziert, davon 2 in der Gruppe mit CHT (8 %) und 4 in der mit CHT + BEV (40 %). GU-Fisteln entwickelten sich ausschließlich in der Gruppe mit CHT + BEV (3/4; 75 %). Von den 6 Patientinnen (83 %) mit Fistelbildung hatten 5 eine vorangehende invasive diagnostische Abklärung und 1 Patientin wurde einer neuerlichen Radiotherapie unterzogen. Ein Lokalrezidiv hatten 3/6 Patientinnen entwickelt. Weitere Risikofaktoren für die Entwicklung einer Fistel konnten nicht identifiziert werden.
Schlussfolgerung
Die zusätzliche Gabe von BEV zur CHT bei RecCC-Patienten, die primär mit IGABT und RCHT behandelt wurden, könnte möglicherweise zu einer erhöhten Rate an GU-Fisteln führen. Zukünftige Studien sollten Risikofaktoren für Fistelbildung untersuchen, um eine gründliche Patientenselektion für die Gabe von BEV bei RecCC zu ermöglichen.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
For patients with locally advanced cervical cancer (LACC), concurrent radiochemotherapy including brachytherapy (BT) is the standard therapy, leading to good oncologic results [1,2,3]. The reported absolute risk of developing grade 3–4 (G3–4) genitourinary (GU) or gastrointestinal (GI) fistulae through definitive radiation therapy including standard BT with dose prescription to point A is around 9% (overall G3–4 toxicity 30%) [4]. Within the last few years, modern radiotherapy techniques have been introduced into the treatment of LACC. These include magnetic resonance (MR) image-guided adaptive brachytherapy (IGABT) [5] with dose prescription individualised to the target at the time of BT. In a recently published cohort of 731 patients, the overall actuarial rate of G3–4 GI and GU toxicity after definitive radiochemotherapy and IGABT was 11% at 5 years [6, 18]. A previous publication from our centre on 156 patients in whom systematic IGABT was performed reported only 2/156 fistula events [5]. Despite excellent overall local tumour control results, several series [5, 7, 8] still observed relatively high rates of distant recurrences after IGABT, especially in patients with advanced stage (stage III/IV) and/or nodal disease [6]. These distant metastases require cytotoxic treatment.
Patients with recurrent cervical cancer (RecCC), depending on the site of relapse (local, distant), have been treated by systemic chemotherapy (CHT), typically with paclitaxel-containing regimes. Since 2014, the use of bevacizumab (BEV) in combination with systemic CHT for the treatment of recurrent or metastatic cervical cancer has become common. It has been shown that the addition of BEV was associated with a significant increase in progression-free and overall survival [9]. However, it has also been reported that CHT+BEV is associated with an increased risk of fistula formation when compared to CHT alone in patients with cervical cancer [10], even in the absence of radiation treatment. In a subset analysis of the Gynecologic Oncology Group trial (GOG 240) published in abstract form [11], it was observed that among the patients who developed GI vaginal fistula, 100% had received prior pelvic radiation, some including standard brachytherapy. However, little is known about the risk factors for fistula formation in the presence of BEV. This study aims to evaluate whether patients with RecCC treated initially by concurrent radiochemotherapy and IGABT have an increased risk for GI and GU fistula formation after CHT+BEV treatment.
Materials and methods
Patients
Consecutive patients diagnosed with RecCC who were treated between 2009 and 2014 in our institution were enrolled in this study. Clinical data were obtained using available tumour databases and by electronic chart review. The 2009 International Federation of Gynecology and Obstetrics (FIGO) classification system was used [12]. Eligible patients had recurrence of a formerly locally advanced cervical cancer that had been initially treated by definitive concurrent radiochemotherapy including IGABT in our institution. Patients treated initially with surgery or those with primary metastatic disease were not eligible.
Tumour status was assessed, the presence of GU and GI fistula identified, and survival and follow-up times were recorded. Risk factors for fistula development including comorbidities (diabetes, arterial hypertension, peripheral vascular disease, thromboembolic events), previously performed bowel surgery, minor interventions/biopsy/major pelvic surgery after RecCC and number of treatment cycles were documented.
The primary endpoint was to document the frequency of fistula events in both groups (CHT or CHT+BEV) in this mono-institutional series.
The Ethics Committee of our institution gave approval prior to initiation of the study (IRB approval number: 1996/2015). All patients consented to treatment according to institutional guidelines, as well as to anonymized assessments and analysis of data and outcome of therapy. Records were anonymized and de-identified prior to analysis.
Treatment
Initial treatment
All patients received definitive concurrent radiochemotherapy. Radiotherapy consisted of external beam radiotherapy (EBRT) concurrent with weekly cisplatin-based CHT (usually cisplatin 5 × 40 mg/m2 body surface area) and IGABT. The maximally allowed duration of radiation therapy was 50 days in total.
External beam radiotherapy
EBRT was delivered using three-dimensional conformal techniques or intensity-modulated radiation therapy. The clinical target volume (CTV) irradiated through EBRT consisted of the tumour, entire uterus, bilateral parametria, upper vagina (if no vaginal involvement had been present) and the pelvic lymph nodes. In case of lymph node involvement of the common iliac or para-aortic (PAN) lymph nodes (as diagnosed by positron-emission tomography/CT [PET-CT] or laparoscopic staging lymphadenectomy), para-aortic radiotherapy was performed. The prescribed dose was 45 Gy at 1.8 Gy per fraction. Grossly involved lymph nodes, if not surgically removed, were treated with an additional boost (range 55–60 Gy).
Image-guided adaptive brachytherapy
Systematically, MRI-based IGABT was performed in all patients diagnosed with LACC with definitive intent. The high-risk CTV (HRCTV) and/or the intermediate-risk CTV (IRCTV) was contoured according to Gyn GEC-ESTRO Recommendations I [13]. Organs at risk (OARs) were contoured: rectum, sigmoid colon and urinary bladder. Dose–volume histogram (DVH) parameters for the HRCTV, IRCTV and OARs were calculated and reported according to Gyn GEC-ESTRO Recommendations II [14]. Dose prescription for target and dose constraints for OARs were applied according to our institutional guidelines [5]. Our planning aim was ≥85 Gy to 90% of the HRCTV (D90). This total EQD2 (equivalent dose in 2 Gy per fraction) from EBRT and BT was calculated using an a/β of 10 Gy for tumour (EQD210) and 3 Gy for OARs (EQD23) [15].
Follow-up
All patients were followed-up in a joint programme by a gynaecologic oncologist and a radiation oncologist specialised in gynaecologic malignancies. Regular follow-up included clinical examination, blood analysis and imaging. Complete remission after initial treatment was defined as the absence of disease in the cervix (uterus), upper vagina, parametrium and regional lymph nodes, as verified by clinical examination, abdominal and thoracic imaging, and biopsy as appropriate. Patients were followed-up every 3 to 4 months for the first 3 years, every 6 months for the following 2 years and annually up to 10 years and beyond thereafter. Follow-up was performed at our institution using standardized questionnaires and assessment forms.
If recurrent disease was suspected, restaging by CT scans of the thorax and abdomen as well as MRI of the pelvis was performed. Whenever possible, recurrent disease was confirmed by biopsy and PET-CT was additionally performed.
Recurrence treatment
Chemotherapy/bevacizumab
Within this study, all patients were treated by either CHT or CHT+BEV. In addition, salvage surgery was performed in selected cases. CHT consisted of paclitaxel in combination with cisplatin (n = 18), with carboplatin (n = 2), or with topotecan (n = 5). Alternatively, selected patients received cisplatin in combination with topotecan (n = 9) or carboplatin with docetaxel (n = 1). CHT was administered until progression, complete response or treatment-limiting toxicity occurred. Starting 2013, most patients received BEV in addition to CHT (n = 10). Thereafter, patients were again followed-up according to the institution’s follow-up program. In a few cases, salvage surgery or radiotherapy of metastases was performed in the presence of oligometastases in lung, liver or periaortic nodes.
Statistical analysis
Time-to-event analyses were computed using the Kaplan–Meier method and log-rank test, with and IBM SPSS 23.0 for MAC (SPSS 23.0, IBM Inc., Armonk, NY, USA). Time intervals for survival analyses were calculated from the date of biopsy to the date of event or last follow-up. Patients lost to follow-up were censored at the time of last follow-up.
Descriptive statistic values are given as mean (standard deviation, SD). T-tests and χ2 tests were used to compare patients’ characteristics and risk factors for fistula formation between groups. P-values <0.05 were considered statistically significant. Overall survival was analysed using the log-rank test.
Results
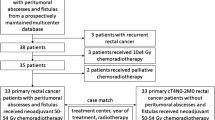
A total of 35 patients were included in this study. Patients’ and treatment characteristics are shown in Table 1. There were no fistulae at the time of relapse diagnostic. CHT was received by 25 patients and 10 patients received CHT+BEV. Patient characteristics and treatment modalities in the both groups were similar. All 10 patients in the CHT +BEV group had undergone interstitial IGABT as opposed to 21/25 in the CHT group (p = 0.18).
Table 2 provides treatment details of the therapy at first diagnosis and the number of events analysed according to the type of treatment at recurrence. No statistically significant difference in radiation dose (90.4 Gy vs. 89.4 Gy, p = 0.353) or number of CHT cycles at RecCC (5.1 vs. 6.4, p = 0.403) was observed between treatment groups.
A total of six fistulae were recorded (patient tumour and treatment details in Table 3: P1-6). In the CHT+BEV group, a significantly higher rate of fistula formation (4/10 patients, 40%) was observed compared to the CHT only group (2/25 patients, 8%; p = 0.043).
GU fistula formation was noticed only in the CHT+BEV group (3/10 patients), of which two were grade 2 and one was grade 3 requiring surgical intervention [16]. Additionally, a grade 3 rectovaginal fistula was documented in this group (P2). In the CHT only group, both events were rectovaginal fistula grade 3. For all patients with G3 rectovaginal fistula a functional colostomy was performed. For the G3 GU fistula, an ileal conduit was necessary.
At the time of recurrence, 2 patients had persistent local disease (incomplete remission), 1 patient had local recurrence (which was treated with palliative re-irradiation) and 3 patients had systemic recurrence (Table 3).
All 6 patients with fistula formation had undergone an invasive procedure or palliative pelvic radiation prior to or during the systemic palliative treatment (Table 3). In the CHT group the events occurred subsequent to a posterior vaginal wall biopsy (P5) and after pelvic re-irradiation (P3). In this group, a further 10 of the remaining 23 patients had undergone an invasive procedure but did not develop fistula (Table 1). In the CHT+BEV group, 4/4 patients with events (100%) had undergone at least a minimally invasive procedure (i. e. ureter stenting) and only 1/6 patients (17%) did not develop an event after an invasive procedure.
We found no association between radiation dose to the target or the reported DVH parameters for OARs and the rate of fistula (Table 4).
Within the cohort, median follow-up was 11 months (range 0–50 months) and overall survival time from the date of diagnosis of RecCC was 8 months (2–27 months) and 26 months (5–87 months) from diagnosis of primary disease. Fistula formation had no significant impact on overall survival (p = 0.317).
Discussion
In this study, patients receiving a combination of CHT and BEV for the treatment of RecCC had a significantly higher risk for fistula formation than patients receiving CHT alone (40 vs. 8%). We observed a notably higher rate of GU fistula in patients treated with CHT+BEV (30% vs. none). The rate of rectovaginal fistula was similar in the two groups (10 vs. 8%).
Previously published studies reported an overall fistula (>grade 2) formation rate of 8.6% (GI vaginal) and 3.2% GI perforation in 218 patients with preliminary metastatic or recurrent cervical cancer treated in the CHT+BEV arm [17] of the GOG 240 study (first data freeze). Furthermore, the rate of fistula (any grade) formation was even higher (12.6%) during CHT+BEV treatment if only patients with prior radiochemotherapy were considered [11]. Overall, GOG 240 reported an increased incidence of 6% of fistula formation (second data freeze) [9]. It is not clear how many patients had received definitive radiochemotherapy including IGABT in the GOG 240 cohort. In our cohort, only patients who received definite IGABT plus radiochemotherapy as initial treatment were included. Therefore, our cohort is the first one comparing CHT and CHT+BEV in LACC patients previously treated with definitive radiochemotherapy and IGABT.
All patients who developed fistulae in our cohort had undergone a minor intervention (5/6, 83%; repeated ureter stenting, biopsy or pelvic re-irradiation) or a major pelvic surgery (1/6, 17%). This is in accordance with the observation of Feddock el al. [19], who associated pelvic radiation and invasive procedures with 8.2% fistula formation, even in the absence of CHT ± BEV. In the CHT group, 43% (10/23) of the non-event patients had undergone an intervention, while in the CHT+BEV only group, 17% (1/6) had undergone an invasive pelvic procedure and did not develop a fistula. This may suggest that BEV in the presence of an invasive pelvic procedure may trigger GU fistula formation. There are case reports in literature suggesting that a combination of perioperative BEV administration and an invasive procedure could result in fistula formation. Aortooesophageal fistula rupture or colovesical fistula during treatment including BEV due to metastatic colorectal cancer have been reported in case studies [25]. One other report describes two late-onset pulmonary fistulae after resection of pulmonary metastasis from colorectal cancer following perioperative CHT with BEV [26]. An increased risk of bowel perforation or fistula formation for patients with recurrent epithelial ovarian cancer treated with BEV has been observed [24, 27, 28].
Although not statistically significant due to the limited number of patients and events, one may observe the fact that 3/6 patients with fistulae had a local recurrence (2 patients never achieved complete local remission and 1 had a local recurrence).
We could not detect any association between comorbidities, radiation dose, performance status or previously performed bowel surgery prior to the diagnosis of RecCC and a higher rate of fistula formation. Our findings are in accordance with previously published reports [20]. In a study including 30 patients with FIGO stage IVA (with bladder or/and rectal infiltration) undergoing radiochemotherapy, the 5‑year fistula-free survival rate was 64%, but no prognostic variables were identified. Although all the patients in the CHT +BEV group underwent interstitial IGABT as opposed to 84% in the CHT group, the use of interstitial implants is not statistically correlated to the occurrence of fistula when BEV is added to the treatment of RecCC (p = 0.18). Moreover, recent literature shows that primarily use of advanced IGABT, especially interstitial implants, does not increase late toxicity when compared to intracavitary therapy only [18].
Recent studies suggest that only intermediate- and high-risk RecCC patients show a survival benefit when receiving CHT+BEV [21]. These patients have 2–3 (intermediate-) and 4–5 (high-risk) risk factors from: black race, performance status 1, pelvic disease, prior cisplatin and progression-free interval <365 days. Hence, patient selection is crucial with respect to side effects and complications. Several approaches were performed to identify biomarkers to predict the effect of BEV on an individual basis [22]. However, no predictive biomarker has been established thus far.
CHT+BEV is administered to RecCC patients without curative intent. The quality of life in this palliative setting is of particular importance and should have a substantial influence on the selection of therapy. Interestingly, while GOG 240 reported an increased rate of fistula in the CHT+BEV group, the quality of life was not decreased in this group. Other reports show that fistula formation leads to a substantial reduction in quality of life [23]. Therefore, patient-reported outcomes, as used in GOG 240, might not be appropriate to determine the detrimental effect of fistula formation on quality of life.
Based on our observations, we suggest that when facing persistent disease or local recurrence, with or without systemic disease, caution should be used in prescribing CHT+BEV. This combination should be offered only after thoroughly informing the patients about the high probability of developing fistula, especially GU fistula. Prudence should also be used when facing ureteral stent change or other pelvic interventions, which are common in patients with RecCC.
Admittedly, the shortcomings of this study have to be considered. This was a retrospective data analysis of a small patient cohort from a single institution. The limited number of patients included in this report impaired statistical analysis and multivariate models were not feasible. However, given the lack of published data and increasing number of patients who are possibly candidates for this treatment, we want to raise awareness about the potential risks of using BEV in addition to CHT in the setting of pelvic RecCC and related interventions.
Conclusion
Until larger studies are available, based on our observations in this small cohort, and given the overall survival benefit [9], CHT+BEV should probably be offered mainly to patients with local control and systemic recurrences. Future clinical studies are required to identify predictive and prognostic factors for fistula formation, in order to improve patient selection for CHT+BEV in the setting of RecCC.
References
Perez CA, Grigsby PW, Chao KS, Mutch DG, Lockett MA (1998) Tumor size, irradiation dose, and long-term outcome of carcinoma of uterine cervix. Int J Radiat Oncol Biol Phys 41:307–317
Eifel PJ, Jhingran A, Brown J, Levenback C, Thames H (2006) Time course and outcome of central recurrence after radiation therapy for carcinoma of the cervix. Int J Gynecol Cancer 16:1106–1111
Chemoradiotherapy for Cervical Cancer Meta-Analysis Collaboration (2008) Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: a systematic review and meta-analysis of individual patient data from 18 randomized trials. Journal of clinical oncology: official journal of the American Society of. J Clin Oncol 26:5802–5812
Kizer NT, Thaker PH, Gao F, Zighelboim I, Powell MA, Rader JS et al (2011) The effects of body mass index on complications and survival outcomes in patients with cervical carcinoma undergoing curative chemoradiation therapy. Cancer 117:948–956
Potter R, Georg P, Dimopoulos JC, Grimm M, Berger D, Nesvacil N et al (2011) Clinical outcome of protocol based image (MRI) guided adaptive brachytherapy combined with 3D conformal radiotherapy with or without chemotherapy in patients with locally advanced cervical cancer. Radiother Oncol 100:116–123
Sturdza A, Potter R, Fokdal LU, Haie-Meder C, Tan LT, Mazeron R et al (2016) Image guided brachytherapy in locally advanced cervical cancer: Improved pelvic control and survival in RetroEMBRACE, a multicenter cohort study. Radiother Oncol. doi: 10.1016/j.radonc.2016.03.011
Gill BS, Kim H, Houser CJ, Kelley JL, Sukumvanich P, Edwards RP et al (2015) MRI-guided high-dose-rate intracavitary brachytherapy for treatment of cervical cancer: the University of Pittsburgh experience. Int J Radiat Oncol Biol Phys 91:540–547
Castelnau-Marchand P, Chargari C, Maroun P, Dumas I, Del Campo ER, Cao K et al (2015) Clinical outcomes of definitive chemoradiation followed by intracavitary pulsed-dose rate image-guided adaptive brachytherapy in locally advanced cervical cancer. Gynecol Oncol 139:288–294
Tewari KS, Sill MW, Long HJ 3rd, Penson RT, Huang H, Ramondetta LM et al (2014) Improved survival with bevacizumab in advanced cervical cancer. N Engl J Med 370:734–743
Burger RA, Brady MF, Bookman MA, Monk BJ, Walker JL, Homesley HD et al (2014) Risk factors for GI adverse events in a phase III randomized trial of bevacizumab in first-line therapy of advanced ovarian cancer: A Gynecologic Oncology Group Study. Journal of clinical oncology : official journal of the American Society of. Clin Oncol 32:1210–1217
Willmott LJ (2014) Gastrointestinal and Genitourinary Fistulae in Women Treated with Chemotherapy with and without Bevacizumab for Advanced and Recurrent Cervical Cancer. International Gynecologic Cancer Society, Melbourne (A NRG Oncology – Gynecologic Group Ancillary Data Study 15th Biennial Meeting of the International Gynecologic Cancer Society)
Benedet JL, Bender H, Jones H 3rd, Ngan HY, Pecorelli S (2000) FIGO staging classifications and clinical practice guidelines in the management of gynecologic cancers. FIGO Committee on Gynecologic Oncology. Int J Gynaecol Obstet 70:209–262
Haie-Meder C, Potter R, Van Limbergen E, Briot E, De Brabandere M, Dimopoulos J et al (2005) Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (I): concepts and terms in 3D image based 3D treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV. Radiother Oncol 74:235–245
Potter R, Haie-Meder C, Van Limbergen E, Barillot I, De Brabandere M, Dimopoulos J et al (2006) Recommendations from gynaecological (GYN) GEC ESTRO working group (II): concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy-3D dose volume parameters and aspects of 3D image-based anatomy, radiation physics, radiobiology. Radiol Oncol 78:67–77
Bentzen SM, Dorr W, Gahbauer R, Howell RW, Joiner MC, Jones B et al (2012) Bioeffect modeling and equieffective dose concepts in radiation oncology – terminology, quantities and units. Radiol Oncol 105:266–268
CTEP (2006) Common Terminology Criteria for Adverse Events v3.0 (CTCAE)
Tewari KS (2014) Abstract LBA26 – final overall survival analysis of the phase III randomized trial of chemotherapy with and without bevacizumab for advanced cervical cancer: a NRG oncology – Gynecologic Oncology Group Study. European Society for Medical Oncology, Madrid
Fokdal L, Sturdza A, Mazeron R, Haie-Meder C, Tan LT, Gillham C et al (2016) Image guided adaptive brachytherapy with combined intracavitary and interstitial technique improves the therapeutic ratio in locally advanced cervical cancer: Analysis from the retroEMBRACE study. Radiol Oncol. doi:10.1016/j.radonc.2016.03.020
Feddock J, Randall M, Kudrimoti M, Baldwin L, Shah P, Weiss H et al (2014) Impact of post-radiation biopsies on development of fistulae in patients with cervical cancer. Gynecol Oncol 133:263–267
Biewenga P, Mutsaerts MA, Stalpers LJ, Buist MR, Schilthuis MS, van der Velden J (2010) Can we predict vesicovaginal or rectovaginal fistula formation in patients with stage IVA cervical cancer? Int J Gynecol Cancer 20:471–475
Tewari KS, Sill MW, Monk BJ, Penson RT, Long HJ 3rd, Poveda A et al (2015) Prospective validation of pooled prognostic factors in women with advanced cervical cancer treated with chemotherapy with/without bevacizumab: NRG oncology/GOG study. Clin Cancer Res 21:5480–5487
Gonzalez-Vacarezza N, Alonso I, Arroyo G, Martinez J, De Andres F, Llerena A et al (2016) Predictive biomarkers candidates for patients with metastatic colorectal cancer treated with bevacizumab-containing regimen. Drug Metabol Personal Ther. doi:10.1515/dmpt-2015-0027
Mohr S, Brandner S, Mueller MD, Dreher EF, Kuhn A (2014) Sexual function after vaginal and abdominal fistula repair. Am J Obstet Gynecol 211:74.e1–74.e6
Cohn DE, Kim KH, Resnick KE, O’Malley DM, Straughn JM Jr. (2011) At what cost does a potential survival advantage of bevacizumab make sense for the primary treatment of ovarian cancer? A cost-effectiveness analysis. J Clin Oncol 29:1247–1251
Koda T, Koike J, Masuhara H, Kurihara A, Shiokawa H, Ushigome M et al (2016) A case of Aortoesophageal fistula rupture due to descending thoracic aortic dissection with recurrent colon cancer during chemotherapy containing bevacizumab. Gan To Kagaku Ryoho 43(12):1815–1817
Kanzaki R, Shintani Y, Inoue M, Kawamura T, Funaki S, Minami M, Okumura M (2017) Late-onset pulmonary fistula after resection of pulmonary metastasis from colorectal cancer following perioperative chemotherapy with bevacizumab. Ann Thorac Cardiovasc Surg. doi:10.5761/atcs.cr.16-00117
Richardson DL, Backes FJ, Hurt JD, Seamon LG, Copeland LJ, Fowler JM, Cohn DE, O’Malley DM (2010) Which factors predict bowel complications in patients with recurrent epithelial ovarian cancer being treated with bevacizumab? Gynecol Oncol 118(1):47–51
Burger RA, Brady MF, Bookman MA, Monk BJ, Walker JL, Homesley HD, Fowler J, Greer BE, Boente M, Fleming GF, Lim PC, Rubin SC, Katsumata N, Liang SX (2014) Risk factors for GI adverse events in a phase III randomized trial of bevacizumab in first-line therapy of advanced ovarian cancer: A Gynecologic Oncology Group Study. J Clin Oncol 32(12):1210–1217. doi:10.1200/JCO.2013.53.6524
Acknowledgements
Open access funding provided by Medical University of Vienna.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
A. Sturdza, S. Hofmann, M. Kranawetter, S. Polterauer, C. Grimm, M. Krainer, C. Kirisits, R. Pötter, A. Reinthaller and R. Schwameis declare that they have no competing interests.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Sturdza, A., Hofmann, S., Kranawetter, M. et al. Increased genitourinary fistula rate after bevacizumab in recurrent cervical cancer patients initially treated with definitive radiochemotherapy and image-guided adaptive brachytherapy. Strahlenther Onkol 193, 1056–1065 (2017). https://doi.org/10.1007/s00066-017-1178-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-017-1178-x