
Abstract
Introduction
For high-dose radiation therapy (RT) of prostate cancer, image-guided (IGRT) and intensity-modulated RT (IMRT) approaches are standard. Less is known regarding comparisons of different IGRT techniques and the resulting residual errors, as well as regarding their influences on dose distributions.
Patients and methods
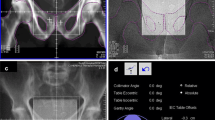
A total of 58 patients who received tomotherapy-based RT up to 84 Gy for high-risk prostate cancer underwent IGRT based either on daily megavoltage CT (MVCT) alone (n = 43) or the additional use of gold markers (n = 15) under routine conditions. Planned Adaptive (Accuray Inc., Madison, WI, USA) software was used for elaborated offline analysis to quantify residual interfractional prostate positioning errors, along with systematic and random errors and the resulting safety margins after both IGRT approaches. Dosimetric parameters for clinical target volume (CTV) coverage and exposition of organs at risk (OAR) were also analyzed and compared. Interfractional as well as intrafractional displacements were determined.
Results
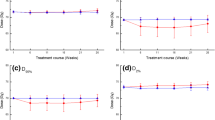
Particularly in the vertical direction, residual interfractional positioning errors were reduced using the gold marker-based approach, but dosimetric differences were moderate and the clinical relevance relatively small. Intrafractional prostate motion proved to be quite high, with displacements of 1–3 mm; however, these did not result in additional dosimetric impairments.
Conclusion
Residual interfractional positioning errors were reduced using gold marker-based IGRT; however, this resulted in only slightly different final dose distributions. Therefore, daily MVCT-based IGRT without markers might be a valid alternative.
Zusammenfassung
Einführung
Bei der hochdosierten Bestrahlung des Prostatakarzinoms sind die bildgesteuerte (IGRT) und die intensitätsmodulierte Bestrahlung (IMRT) Standard. Offene Fragen gibt es beim Vergleich von IGRT-Techniken im Hinblick auf residuelle Fehler und Beeinflussungen der Dosisverteilung.
Methoden und Patienten
Bei 58 Patienten, deren Hochrisiko-Prostatakarzinom am Tomotherapie-System bis 84 Gy bestrahlt wurde, durchliefen die IGRT entweder routinemäßig basierend auf einem alleinigen Megavolt-CT (MVCT; n = 43) oder zusätzlich unter Ausnutzung implantierter Goldmarker (n = 15). Die Software Planned Adaptive (Accuray Inc., Madison, WI, USA) wurde für eine Offline-Analyse eingesetzt, um residuelle Verschiebungen, daraus resultierende systematische und zufällige Fehler sowie Sicherheitssäume für die beiden IGRT-Verfahren zu vergleichen. Außerdem wurden dosimetrische Parameter für die Abdeckung des klinischen Zielvolumens (CTV) und Expositionen von Risikoorganen (OAR) analysiert und verglichen. Inter- und intrafraktionelle Verschiebungen wurden bestimmt.
Ergebnisse
Residuelle interfraktionelle Verschiebungen werden unter Ausnutzung von Goldmarkern insbesondere in dorsaler Richtung reduziert. Die dosimetrischen Verbesserungen sind allerdings moderat und in ihrer klinischen Relevanz überschaubar. Intrafraktionelle Prostataverschiebungen sind mit 1–3 mm hoch, führen aber zu keinen wesentlichen dosimetrischen Verschlechterungen.
Schlussfolgerung
Interfraktionelle residuelle Positionsfehler können mit Hilfe einer goldmarkerbasierten IGRT reduziert werden. Aufgrund der geringen Differenz in den Dosisverteilungen ist jedoch eine IGRT mit täglicher MVCT ohne Marker eine valide Alternative.
Similar content being viewed by others

References
Viani GA, Stefano EJ, Afonso SL (2009) Higher-than-conventional radiation doses in localized prostate cancer treatment: a meta-analysis of randomized, controlled trials. Int J Radiat Oncol Biol Phys 74(5):1405–1418
Zietman AL, DeSilvio ML, Slater JD, Rossi CJ, Miller DW, Adams JA, Shipley WU (2005) Comparison of conventional-dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate: a randomized controlled trial. JAMA 294(10):1233–1239
Frenzel T, Kruell A (2015) The use of IMRT in Germany. Strahlenther Onkol 191(11):821–826
Ghadjar P, Gwerder N, Manser P, Vock J, Madlung A, Mini R, Aebersold DM (2010) High-dose (80 Gy) intensity-modulated radiation therapy with daily image-guidance as primary treatment for localized prostate cancer. Strahlenther Onkol 186(12):687–692
Zelefsky MJ, Kollmeier M, Cox B, Fidaleo A, Sperling D, Pei X, Carver B, Coleman J, Lovelock M, Hunt M (2012) Improved clinical outcomes with high-dose image guided radiotherapy compared with non-IGRT for the treatment of clinically localized prostate cancer. Int J Radiat Oncol Biol Physics 84(1):125–129
Kupelian PA, Langen KM, Willoughby TR, Zeidan OA, Meeks SL (2008) Image-guided radiotherapy for localized prostate cancer: treating a moving target. Semin Radiat Oncol 18(1):58–66
Ghadjar P, Gwerder N, Madlung A, Behrensmeier F, Thalmann GN, Mini R, Aebersold DM (2009) Use of gold markers for setup in image-guided fractionated high-dose-rate brachytherapy as a monotherapy for prostate cancer. Strahlenther Onkol 185(11):731–735
Rudat V, Nour A, Hammoud M, Alaradi A, Mohammed A (2016) Image-guided intensity-modulated radiotherapy of prostate cancer. Strahlenther Onkol 192(2):109–117
Drozdz S, Schwedas M, Salz H, Foller S, Wendt TG (2016) Prostate cancer treated with image-guided helical TomoTherapy® and image-guided LINAC-IMRT. Strahlenther Onkol 192(4):223–231
Graf R, Boehmer D, Nadobny J, Budach V, Wust P (2012) Appropriate patient instructions can reduce prostate motion. Radiat Oncol 7(1):1
Van Herk M (2004) Errors and margins in radiotherapy. Semin Radiat Oncol 14(1):52–64
Moseley DJ, White EA, Wiltshire KL, Rosewall T, Sharpe MB, Siewerdsen JH, Bissonnette JP, Gospodarowicz M, Warde P, Catton CN, Jaffray DA (2007) Comparison of localization performance with implanted fiducial markers and cone-beam computed tomography for on-line image-guided radiotherapy of the prostate. International Journal of Radiation Oncology* Biology. Physics (College Park Md) 67(3):942–953
Mayyas E, Chetty IJ, Chetvertkov M, Wen N, Neicu T, Nurushev T, Ren L, Lu M, Stricker H, Pradhan D, Movsas B (2013) Evaluation of multiple image-based modalities for image-guided radiation therapy (IGRT) of prostate carcinoma: a prospective study. Med Phys 40(4):041707
ICRU (2010) Prescribing, recording, and reporting photon-beam intensity-modulated radiation therapy (IMRT). J ICRU 10(1):83
Walz J, Epstein JI, Ganzer R, Graefen M, Guazzoni G, Kaouk J, Menon M, Mottrie A, Myers RP, Patel V, Tewari A (2016) A critical analysis of the current knowledge of surgical anatomy of the prostate related to optimisation of cancer control and preservation of continence and erection in candidates for radical prostatectomy: an update. Eur Urol 70(2):301–311
Zelefsky MJ, Fuks Z, Happersett L, Lee HJ, Ling CC, Burman CM, Hunt M, Wolfe T, Venkatraman ES, Jackson A, Skwarchuk M (2000) Clinical experience with intensity modulated radiation therapy (IMRT) in prostate cancer. Radiother Oncol 55(3):241–249
Alicikus ZA, Yamada Y, Zhang Z, Pei X, Hunt M, Kollmeier M, Cox B, Zelefsky MJ (2011) Ten-year outcomes of high-dose, intensity‐modulated radiotherapy for localized prostate cancer. Cancer 117(7):1429–1437
Bortfeld T, Webb S (2008) Single-arc IMRT? Phys Med Biol 54(1):N9
Li JS, Lin MH, Buyyounouski MK, Horwitz EM, Ma CM (2013) Reduction of prostate intrafractional motion from shortening the treatment time. Phys Med Biol 58(14):4921–4932
Cramer AK, Haile AG, Ognjenovic S, Doshi TS, Reilly WM, Rubinstein KE, Nabavizadeh N, Nguyen T, Meng LZ, Fuss M, Tanyi JA (2013) Real-time prostate motion assessment: image-guidance and the temporal dependence of intra-fraction motion. BMC Med Physics 13(1):1
Langen KM, Lu W, Willoughby TR, Chauhan B, Meeks SL, Kupelian PA, Olivera G (2009) Dosimetric effect of prostate motion during helical tomotherapy. Int J Radiat Oncol Biol Physics 74(4):1134–1142
Adamson J, Wu Q, Yan D (2011) Dosimetric effect of intrafraction motion and residual setup error for hypofractionated prostate intensity-modulated radiotherapy with online cone beam computed tomography image guidance. Int J Radiat Oncol Biol Physics 80(2):453–461
Ghilezan MJ, Jaffray DA, Siewerdsen JH, Van Herk M, Shetty A, Sharpe MB, Jafri SZ, Vicini FA, Matter RC, Brabbins DS, Martinez AA (2005) Prostate gland motion assessed with cine-magnetic resonance imaging (cine-MRI). Int J Radiat Oncol Biol Physics 62(2):406–417
Nijkamp J, Pos FJ, Nuver TT, De Jong R, Remeijer P, Sonke JJ, Lebesque JV (2008) Adaptive radiotherapy for prostate cancer using kilovoltage cone-beam computed tomography: first clinical results. Int J Radiat Oncol Biol Physics 70(1):75–82
Engels B, Soete G, Verellen D, Storme G (2009) Conformal arc radiotherapy for prostate cancer: increased biochemical failure in patients with distended rectum on the planning computed tomogram despite image guidance by implanted markers. Int J Radiat Oncol Biol Physics 74(2):388–391
Engels B, Soete G, Gevaert T, Storme G, Michielsen D, De Ridder M (2014) Impact of planning target volume margins and rectal distention on biochemical failure in image-guided radiotherapy of prostate cancer. Radiother Oncol 111(1):106–109
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
P. Wust, M. Joswig, R. Graf, D. Böhmer, M. Beck, T. Barelkowski, V. Budach, and P. Ghadjar declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Wust, P., Joswig, M., Graf, R. et al. Dosimetric implications of inter- and intrafractional prostate positioning errors during tomotherapy. Strahlenther Onkol 193, 700–706 (2017). https://doi.org/10.1007/s00066-017-1141-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-017-1141-x