
Abstract
Background and Purpose
In external beam radiotherapy of prostate cancer, the consideration of various systematic error types leads to wide treatment margins compromising normal tissue tolerance. We investigated if systematic set-up errors can be reduced by a set of initial image-guided radiotherapy (IGRT) sessions.
Patients and Methods
27 patients received daily IGRT resulting in a set of 882 cone-beam computed tomographies (CBCTs). After matching to bony structures, we analyzed the dimensions of remaining systematic errors from zero up to six initial IGRT sessions and aimed at a restriction of daily IGRT for 10% of all patients. For threshold definition, we determined the standard deviations (SD) of the shift corrections and selected patients out of this range for daily image guidance. To calculate total treatment margins, we demanded for a cumulative clinical target volume (CTV) coverage of at least 95% of the specified dose in 90% of all patients.
Results
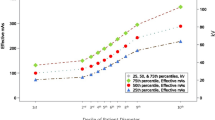
The gain of accuracy was largest during the first three IGRTs. In order to match precision and workload criteria, thresholds for the SD of the corrections of 3.5 mm, 2.0 mm and 4.5 mm in the left-right (L-R), cranial-caudal (C-C), and anterior-posterior (A-P) direction, respectively, were identified. Including all other error types, the total margins added to the CTV amounted to 8.6 mm in L-R, 10.4 mm in C-C, and 14.4 mm in A-P direction.
Conclusion
Only initially performed IGRT might be helpful for eliminating gross systematic errors especially after virtual simulation. However, even with daily IGRT performance, a substantial PTV margin reduction is only achievable by matching internal markers instead of bony anatomical structures.
Zusammenfassung
Hintergrund
Bei der Teletherapie des Prostatakarzinoms führt die Berücksichtigung verschiedener systematischer Fehler zu großen Sicherheitsrändern auf Kosten der Normalgewebetoleranz. Wir untersuchten, inwieweit systematische Lagerungsfehler durch initiale bildgeführte Radiotherapie (IGRT) reduziert werden können.
Patienten und Methodik
Es wurden 882 Cone-Beam-Comutertomographien (CBCT) von insgesamt 27 Patienten analysiert. Nach der Korrektur auf knöcherne Strukturen wurde das Ausmaß des Lagerungsfehlers als gemittelter Wert der Verschiebungen nach null bis sechs CBCTs untersucht. Aus den Standardabweichungen (SD) der Verschiebungen wurden Schwellwerte für maximal 10% aller Patienten definiert, die tägliche Bildführung erhalten sollten. Für die Berechnung der Sicherheitsränder für das Planzielvolumen (PTV) forderten wir eine mindestens 95%ige kumulative Dosisabdeckung des klinischen Zielvolumens bei 90% der Patienten.
Ergebnisse
Drei CBCT stellten den optimalen Kompromiss zwischen Arbeitsbelastung und erzielbarer Genauigkeit durch initiale Bildführung dar (Tabelle 1). Die Schwellwerte für die SD, ab denen wir tägliche IGRT forderten, betrugen 3,5 mm in Links-rechts-(L-R-), 2,0 mm in kranial-kaudaler (C-C-) und 4,5 mm in anterior-posteriorer (A-P-)Richtung (Abbildung 1). Unter Berücksichtigung aller anderen Fehlertypen (Tabelle 2) wurden für das PTV kumulative Sicherheitsränder von L-R 8,6 mm, C-C 10,4 mm und A-P 14,4 mm ermittelt (Tabelle 3, Abbildung 2).
Schlussfolgerung
Ausschließlich initial durchgeführte Bildführung mag zwar größere systematische Fehler, speziell nach virtueller Simulation, kompensieren, eine deutliche Reduktion der PTV-Sicherheitsränder ist aber selbst bei täglicher IGRT nur durch Abgleich auf interne Marker anstelle von knöchernen Strukturen möglich.
Similar content being viewed by others


References
de Boer JCJ, Heijmen BJM. A protocol for the reduction of systematic patient set-up errors with minimal portal imaging workload. Int J Radiat Oncol Biol Phys 2001;50:1350–1365.
de Boer JCJ, van Os MJH, Jansen PP. Application of the no action level (NAL) protocol to correct for prostate motion based on electronic portal imaging of implanted markers. Int J Radiat Oncol Biol Phys 2005;61:969–983.
Deutschmann H, Steininger P, Nairz O, et al., “Augmented Reality” in conventional simulation by projection of 3D structures into 2D images — a comparison with virtual methods. Strahlenther Onkol 2008;184:93–99.
Elsayed H, Bölling T, Moustakis C, et al. Organ movements and dose exposures in teletherapy of prostate cancer using a rectal balloon. Strahlenther Onkol 2007;183:617–624.
Guckenberger M, Meyer J, Wilbert J, et al. Precision of Image-Guided Radiotherapy (IGRT) in six degrees of freedom and limitations in clinical practice. Strahlenther Onkol 2007;183:307–313.
Graham J, Gee A, Hilton S, et al. Geometric uncertainties in radiotherapy of the prostate and bladder. In: McKenzie A et al. Geometric Uncertainties in Radiotherapy — Defining the Planning Target Volume. British Institute of Radiology, London 2003:89–108.
Harrison A, McKenzie A. Standard deviation of a top-hat function. In: McKenzie A et al. Geometric Uncertainties in Radiotherapy — Defining the Planning Target Volume. British Institute of Radiology, London 2003:35.
Hristov DH, Fallone BG. A grey-level image alignment algorithm for registration of portal images and digitally reconstructed radiographs. Med Phys 1996;23:75–84.
Jaffray DA, Drake DG, Moreau M, et al. A radiographic and tomographic imaging system integrated into a medical linear accelerator for localization of bone and soft-tissue targets. Int J Radiat Oncol Biol Phys 1999;45:773–789.
Jaffray DA, Siewerdsen JH, Wong JW, et al. Flat-panel cone-beam computed tomography for image-guided radiation therapy. Int J Radiat Oncol Biol Phys 2002;53:1337–1349.
Jereczek-Fossa BA, Cattani F, Garibaldi C, et al. Transabdominal ultrasonography, computed tomography and electronic portal imaging for 3-dimensional conformal radiotherapy for prostate cancer. Strahlenther Onkol 2007;183:610–616
Keall PJ, Lauve AD, Hagan MP, Siebers JV. A strategy to correct for intrafraction target translation in conformal prostate radiotherapy: simulation results. Med Phys 2007;34:1944–1951.
Langen KM, Jones DTL. Organ motion and its management. Int J Radiat Oncol Biol Phys 2001;50:265–278.
Lauve AD, Siebers JV, Crimaldi AJ, et al. A dynamic compensation strategy to correct patient-positioning errors in conformal prostate radiotherapy. Med Phys 2006;33:1879–1887.
Litzenberg D, Dawson LA, Sandier H, et al. Daily prostate targeting using implanted radiopaque markers. Int J Radiat Oncol Biol Phys 2002;3:699–703.
McKenzie AL, van Herk M, Mijnheer B. The width of margins in radiotherapy, treatment plans. Phys Med Biol 2000;45:3331–3342.
Meeks SL, Harmon JF Jr., Langen KM, et al. Performance characterization of megavoltage computed tomography imaging on a helical tomotherapy unit. Med Phys 2005;32:2673–2681.
Polat B, Wilbert J, Baier K, et al. Nonrigid patient setup errors in the head-and-neck region. Strahlenther Onkol 2007;183:506–511.
Sterzing F, Herfarth K, Debus J. IGRT with helical tomotherapy — effort and benefit in clinical routine. Strahlenther Onkol 2007;183 (Sondernr. 2):35–37.
Sterzing F, Schubert K, Sroka-Perez G, et al. Helical tomotherapy — Experiences of the First 150 Patients in Heidelberg. Strahlenther Onkol 2008;184:8–14.
Van den Heuvel F, Powell T, Seppi E, et al. Independent verification of ultrasound based image-guided radiation treatment, using electronic portal imaging and implanted gold markers. Med Phys 2003;30:2878–2887.
van der Heide UA, Kotte ANTJ, Homan Dehnad H et al. Analysis of fiducial marker-based position verification in the external beam radiotherapy of patients with prostate cancer. Radiotherapy and Oncology 2007;82:38–45.
van Herk M. Errors and Margins in Radiotherapy. Semin Radiat Oncol 2004;4:52–64.
van Herk M, Remeijer P, Rasch C, Lebesque JV. The probability of correct target dosage: dose-population histograms for deriving treatment margins in radiotherapy. Int J Radiat Oncol Biol Phys 2000;47:1121–1135.
Vigneault E, Pouliot J, Laverdie’re J, Roy J, et al. Electronic portal imaging device detection of radioopaque markers for the evaluation of prostate position during megavoltage irradiation: a clinical study. Int J Radiat Oncol Biol Phys 1997;37:205–212.
Wu J, Haycocks T, Alasti H, et al. Positioning errors and prostate motion during conformal prostate radiotherapy using on-line isocentre set-up verification and implanted prostate markers. Radiother Oncol 2001;61:127–133.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nairz, O., Merz, F., Deutschmann, H. et al. A strategy for the use of image-guided radiotherapy (IGRT) on linear accelerators and its impact on treatment margins for prostate cancer patients. Strahlenther Onkol 184, 663–667 (2008). https://doi.org/10.1007/s00066-008-1874-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-008-1874-7