
Abstract
Objective
Anatomic reconstruction of proximal ulna and olecranon fractures allowing early mobilization and prevention of ulnohumeral arthritis.
Indications
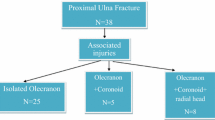
Comminuted olecranon or proximal ulna fractures (including Monteggia fractures), olecranon fractures extending distally from the coronoid process, nonunions of the proximal ulna, segmental fractures of the proximal ulna extending into the shaft, fractures of the proximal ulna associated with a coronoid fracture.
Contraindications
Patients in poor general condition.
Soft-tissue defects around the elbow preventing wound closure over the plate.
Pediatric fractures with open growth plates where screws would cross the physis.
Surgical Technique
Posterior approach to the elbow. Hinging the fracture site open by extension of the proximal fragment based on triceps insertion. Fracture involvement of the coronoid with a large displaced fracture fragment can generally be reduced through the fracture side. Reconstruction with temporary Kirschner wires. Fixation by placing a (precontoured) plate around the tip of the olecranon with a long intramedullary screw and orthogonal (uni)cortical screws in the shaft. Radial head pathology can be addressed – if needed – through the same incision. Internal fixation, resection or prosthetic replacement of the radial head is done based on injury pattern/stability.
Postoperative Management
Functional rehabilitation using active assisted range of motion of the elbow may be started immediately out of splint. Posterior splint for 7–10 days to allow wound healing.
Results
Between 2003 and July 2008, 26 patients were treated with posterior plating of the proximal ulna and olecranon using this strategy. There were 23 acute fractures (of which one was referred for revision after suboptimal fixation a few days earlier), one nonunion that became traumatized, and two nascent malunions. A midline posterior approach allowed addressing both ulna and radial head pathology. The plate was contoured to wrap around the olecranon. All fractures healed. There were one postoperative infection, one transient ulnar neuropathy, one transient radial neuropathy, and one nonresolving ulnar/median neuropathy in a complex upper extremity injury. At follow-up after an average of 18 months, range of motion was on average 132°/18° of flexion/extension, and 75°/70° of pronation/supination. All fractures had healed at an average of 4.8 months. Ten patients had their hardware removed.
Zusammenfassung
Operationsziel
Anatomische Rekonstruktion von Frakturen der proximalen Ulna und des Olekranons mit früher Mobilisation und Vermeidung einer ulnohumeralen Arthrose.
Indikationen
Trümmerfrakturen des Olekranons oder proximale Ulnafrakturen (inklusive Monteggia-Frakturen), Olekranonfrakturen distal des Processus coronoideus, Pseudarthrosen der proximalen Ulna, Stückbrüche der proximalen Ulna mit Ausläufern in den Schaft, Frakturen der proximalen Ulna mit begleitender Fraktur des Processus coronoideus.
Kontraindikationen
Schlechter Allgemeinzustand des Patienten.
Weichteildefekt am Ellenbogen, welcher den Wundverschluss über der Platte verhindert.
Frakturen im Wachstumsalter, bei denen die Schrauben die Epiphyse kreuzen würden.
Operationstechnik
Posteriorer Zugang zum Ellenbogen. Aufklappen der Fraktur am proximalen, den Trizepsansatz tragenden Fragment. Eine Frakturbeteiligung des Processus coronoideus mit großem disloziertem Fragment kann normalerweise über die Bruchstelle reponiert werden. Temporäre Fixation mit Kirschner-Drähten. Anbringen einer vorgeformten Platte um die Olekranonspitze mit langer intramedullärer Schraube und orthogonaler (uni)kortikaler Schraube in den Schaft. Frakturen des Radiusköpfchens können nötigenfalls über den gleichen Zugang behandelt werden. Interne Fixation, Resektion oder prothetische Versorgung des Radiusköpfchens je nach Verletzungsmuster und Stabilität.
Weiterbehandlung
Funktionelle Rehabilitation mit aktiv-assistierten Bewegungsübungen des Ellenbogens aus der Schiene heraus. Dorsale Schiene für 7–10 Tage bis zur Wundheilung.
Ergebnisse
Zwischen 2003 und Juli 2008 wurden 26 Patienten mit hinterer Verplattung der proximalen Ulna und des Olekranons nach dieser Strategie behandelt. Es handelte sich um 23 frische Frakturen (wovon ein Patient zur Revision einige Tage nach auswärts erfolgter suboptimaler Fixation zugewiesen wurde), eine lang bestehende Pseudarthrose sowie zwei entstehende Fehlverheilungen. Ein hinterer medianer Zugang erlaubte die Behandlung sowohl von Pathologien der Ulna als auch des Radiusköpfchens. Die Platte war vorgeformt, um sich um das Olekranon zu legen. Alle Frakturen verheilten. Es kam zu einer postoperativen Infektion, je einer vorübergehenden ulnaren und radialen Neuropathie sowie einer anhaltenden ulnomedianen Neuropathie bei komplexer oberer Extremitätenverletzung. Bei der Nachuntersuchung nach durchschnittlich 18 Monaten betrug der durchschnittliche Bewegungsumfang bei Flexion/Extension 132°/18° und bei Pronation/Supination 75°/70°. Alle Frakturen verheilten nach durchschnittlich 4,8 Monaten. Bei zehn Patienten wurden die Implantate entfernt.
Similar content being viewed by others

References
Boyd HB. Surgical exposure of the ulna and proximal third of the radius through one incision. Surg Gynecol Obstet 1940;71:86–7.
Duckworth AD, Kulijdian A, McKee MD. Residual subluxation of the elbow after dislocation or fracture-dislocation: treatment with active elbow exercises and avoidance of varus stress. J Shoulder Elbow Surg 2007;17:276–80.
Fyfe IS, Mossad MM, Holdsworth BJ. Methods of fixation of olecranon fractures. An experimental mechanical study. J Bone Joint Surg Br 1985;67:367–72.
Hak DJ, Golladay GJ. Olecranon fractures: treatment options. J Am Acad Orthop Surg 2000;8:266–75.
Hume MC, Wiss DA. Olecranon fractures. A clinical and radiographic comparison of tension band wiring and plate fixation. Clin Orthop Relat Res 1992;285:229–35.
Jupiter JB, Leibvic SJ, Ribbans W. The posterior Monteggia lesion. J Orthop Trauma 1991;54:395–402.
Nowinski RJ, Nork SE, Segina DN. Comminuted fracture-dislocations of the elbow treated with an AO wrist fusion plate. Clin Orthop Relat Res 2000;378:238–44.
Quintero J, Vareck T. Olecranon, radial head, and complex elbow injuries. In: Ruedi TP, Buckley RE, Moran CG, eds. AO principles of fracture management, vol 2: Specific fractures, 2nd edn. Stuttgart: Thieme, 2007:626–41.
Ring D, Jupiter JB. Fracture-dislocation of the elbow. J Bone Joint Surg Am 1998;80:566–80.
Ring D, Jupiter JB. Compass hinge fixator for acute and chronic instability of the elbow. Oper Orthop Traumatol 2005;17:143–57.
Ring D, Jupiter JB, Sanders RW. Transolecranon fracture-dislocation of the elbow. J Orthop Trauma 1997;11:545–50.
Simpson NS, Goodman LA, Jupiter JB. Contoured LCDC plating of the proximal ulna. Injury 1996;27:411–7.
Wagner M, Frigg R. Radius and ulna, proximal. AO manual of fracture fixation. Internal fixators. Concepts and cases using LCP and LISS. Stuttgart: Thieme, 2006:366–98.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kloen, P., Buijze, G.A. Treatment of Proximal Ulna and Olecranon Fractures by Dorsal Plating. Orthop Traumatol 21, 571–585 (2009). https://doi.org/10.1007/s00064-009-2006-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00064-009-2006-y