
Abstract.
Investigating the signalling pathways that regulate heart development is essential if stem cells are to become an effective source of cardiomyocytes that can be used for studying cardiac physiology and pharmacology and eventually developing cell-based therapies for heart repair. Here, we briefly describe current understanding of heart development in vertebrates and review the signalling pathways thought to be involved in cardiomyogenesis in multiple species. We discuss how this might be applied to stem cells currently thought to have cardiomyogenic potential by considering the factors relevant for each differentiation step from the undifferentiated cell to nascent mesoderm, cardiac progenitors and finally a fully determined cardiomyocyte. We focus particularly on how this is being applied to human embryonic stem cells and provide recent examples from both our own work and that of others.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic heart diseases such as ischemia and hypertensive heart failure are characterized by irreversible loss of cardiomyocytes. Generally accepted paradigms are that adult cardiomyocytes lack the ability to regenerate the myocardium in part because proliferation slows down at the time of birth. Although after birth cardiomyocytes do undergo some rounds of cell division (in human dividing cells are still found up to 3 weeks after birth), the last round of cell division in both human and mouse is actually incomplete. The cells undergo nuclear division only, and as a result the adult cardiomyocytes either have two diploid nuclei or one tetraploid nucleus. In addition, the heart was considered to lack stem cells. However, several recent reports [1–3] have described resident stem cell populations in human and rodent hearts that proliferate and may give rise to cardiomyocytes, vascular smooth muscle cells and endothelial cells.
Nevertheless, the regenerative capacity of the heart is still limited, and cell transplantation for the treatment of cardiac disease remains an attractive concept. Finding the most suitable source of cells for this purpose is, however, a major challenge of experimental cardiology at the present time. Stem cells may be derived either from adult human tissues (‘adult stem cells’) or from human embryos (‘embryonic stem cells’). Both are considered as options deserving further research, although there are ethical reservations on using human embryonic stem cells (HESCs) because their derivation involves destruction of the embryo (reviewed in [4, 5]). Here, we provide a brief introduction to stem cells and the scientific background to current approaches to producing, selecting and identifying the most suitable cells for restoring cardiac function. Many of these are based on the premise that understanding heart development will lead to ways of (re) programming stem cells. The recent literature has been confused by the question of whether adult stem cells, particularly those derived from conventional hematopoietic sources like bone marrow, or umbilical cord blood, can ‘transdifferentiate’ i.e. convert to another lineage by differentiation. The consensus is that bone marrow may have therapeutic benefit but that this is not based on the ability of bone marrow cells to transdifferentiate into cardiomyocytes (reviewed in [6]). We will not consider this in detail here. There are at present two or, possibly, three stem cell sources of bona fide cardiomyocytes: ESCs, resident cardiac progenitor or stem cells in the heart (CPCs or CSCs) and possibly mesenchymal stem cells (MSCs), present in bone marrow, cord blood and adipose tissue. Most strategies used involve inducing differentiation of stem cells in culture to a cardiac phenotype compatible with survival, electromechanical coupling and integration in the host heart tissue, without causing arrythmias. Adult cardiomyocytes do not survive transplantation into the adult heart [7], and skeletal muscle myoblasts are functionally isolated from their host cells, which may lead to arrythmias [8]. However, fetal cardiomyocytes from various species, including humans, do survive transplantation in the heart [9,10], so the goal may be to derive cells with fetal cardiomyocyte phenotype.
An important question is how to obtain these human (fetal) cardiomyocytes in sufficiently large numbers to be of use in therapy. In practice, this might mean ∼108–109 cells being required for each adult patient, the number of cardiomyocytes lost in the left ventricle following a major myocardial infarction in humans. Clearly, deriving them routinely from human fetuses would raise important ethical issues. Alternatives would be to identify and expand cardiac progenitors with the capacity to proliferate ex vivo either from the adult or fetal heart, or derive cardiomyocytes from stem cells at high efficiency. From the adult heart there would be the advantage that the cells could be autologous. For all strategies, understanding how cardiac cell fate is specified by extracellular cues in the embryo, what the molecular signatures are of the intermediate differentiation states of the cardiomyogenic lineage and how the electrical and physiological phenotypes of stem cell-derived cardiomyocytes compare with those of the normal counterparts is essential if cell transplantation therapy is to be used effectively in restoring cardiac function.
Recapitulating the extracellular signals used by the embryo to drive differentiation is currently proving the most fruitful strategy to control the differentiation of stem cells to selected lineages [11,12]. By contrast, ectopic expression of lineage-associated or -specific transcription factors has met with relatively little success even in mESCs; it appears that signal timing, duration and dose are much more subtle than can be achieved by the relatively crude method of gene overexpression. Here we consider possible stem cell sources of cardiomyocytes for cardiac repair, review the signals thought to control allocation of pluripotent cells first to the nascent mesoderm lineages during gastrulation, then their subsequent development into cardiac progenitors and fully differentiated cardiomyocytes (Fig. 1). We begin, however, with a short description of heart development in mammals.

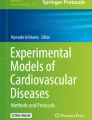
A model of embryonic stem cell differentiation towards the cardiomyocyte lineage based on current mouse ESC differentiation methods. Pluripotent ESCs are maintained through transcription factors Oct-4, Nanog and Sox-2. Given appropriate signals from EB culture or a 2D culture system, the cells differentiate into a primitive, pre-hemangioblast type cell with broad mesodermal potential (blue arrow). These cells are characterised by the expression of key transcription factors like brachyury and MESP and may still retain the expression of pluripotency associated genes. From these cells, a Flk-1-positive subpopulation appears with hemangiblast-like differentiation activity highlighted by a robust ability to form blood cells (large orange arrow). However, these cells still retain remarkable plasticity and can give rise to increasingly more restricted Flk-1-positive progenitors (blue arrow). More restricted Flk-1-positive cells may predominantly differentiate into endothelial cells (large orange arrow) and less readily (small orange arrow) to cardiac cells. Immunosorting or magnetic cell separation for Flk-1 and other surface receptors like CXCR4 enables the enrichment of a more defined progenitor cell subpopulation which differentiates predominantly into beating cardiomyocytes (large orange arrow) with a limited capacity to form endothelial cells (small orange arrow).
Differentiation and early morphogenesis in the mammalian heart
Heart formation is initiated in vertebrate embryos soon after gastrulation when the three embryonic germ layers, ectoderm, endoderm and mesoderm, are established in the primitive streak. The heart is derived from the mesoderm and is the first definitive organ to form in development. Its morphogenesis, growth and integrated function are essential for survival of the embryo even by midgestation. Cardiac progenitor cells are for the most part localized in the anterior primitive streak. Different populations of precursor cells are distributed within the streak (in relation to the organizing centre, or node) in the same anterior-posterior order that they are later found in the tubular heart [13]. As a result, cells furthest from the node end up in the atrium, those nearer the node end up in the ventricle whilst those nearest the node later form the outflow tract. In addition to precursors in the primitive streak, there are also precursors bilaterally distributed in the epiblast directly adjacent to the streak. As development proceeds, the precursor population of precardiac mesoderm emigrates from the streak in an antero-lateral direction, giving rise to the heart-forming fields on either side of the streak. These heart fields formed at gastrulation give rise to the left ventricle and possibly the atrioventricular canal (AVC) and part of the atria as well as endocardial progenitor cells. During subsequent development the right ventricle and outflow tract are added from the anterior heart field and the inflow tract from the posterior heart field. The expression of Islet-1 defines two cell populations of which one generates the linear heart tube, i.e. the left ventricle, and the other contributes to the rest of the developing organ [14]. The axial distribution is maintained as the fields migrate to fuse and form the cardiac crescent. Cells of the cardiac crescent then adopt a definitive cardiac fate in response to cues from adjacent anterior endoderm [15]. Anterior endoderm in particular appears to have an instructive function in cardiogenesis in various species (reviewed in [16]). Ablation of anterior endoderm in amphibians results in loss of myocardial specification [17], whilst explants of posterior, blood-forming mesoderm in chick are reprogrammed to express cardiac instead of blood-restricted marker genes if combined with anterior endoderm [18]. After cardiac mesoderm has been specified, it ends up at the ventral side of the embryo where the heart field start to fuse due to folding of the embryo. A single heart tube thus forms. In mutant mouse and zebrafish in which this fails to take place, two tube-like structures form (cardiac bifida) which both acquire contractile activity [19–22]. However, in the GATA4 and miles-apart knockouts the phenotypes are due to folding defects, the heart abnormalities in these cases being secondary events. Some mutants also lack or have defective endodermal tissue [22]. Thus, the endoderm is not only important for differentiation of cardiac precursors but is also essential for cardiac mesoderm migration, although it is clear that tube formation also involves a cell autonomous function of cardiac mesoderm itself.
Once this process of primary cardiac induction is complete, cells are then recruited from lateral plate mesoderm, medial to the primary heart field, to give rise to the secondary, anterior heart field (AHF). The cells recruited contribute to the primitive right ventricle and outflow tract [23]. Whilst the heart tube is initially almost straight, the ventricular segment at this stage starts to bulge ventrally, flips to the right and begins to form a C-shaped heart. Left-right asymmetry thus becomes evident and cardiac looping morphogenesis has commenced. Through a series of ‘ballooning’ steps and morphogenetic movements the four-chambered heart eventually forms [24].
Embryonic and adult stem cells
Stem cells are primitive cells present in all organisms that can divide and give rise to more stem cells or switch to become more specialized cells, such as those of heart, brain, muscle and kidney. Stem cells in early embryos give rise to cells of all tissues of the adult body and are therefore termed pluripotent. Stem cells of adult tissues, involved in tissue replacement and repair, usually give rise only to cell types already present in the surrounding tissues from which they are derived. Restricted differentiation and inability to cross lineage boundaries has led to them being termed multipotent. Stem cells of the bone marrow, for example, give rise to hematopoietic cells.
The first ESCs were isolated 25 years ago from mouse preimplantation embryos 3.5 days after fertilization. The background to the discovery lay in the study of teratocarcinoma, a spontaneous tumour of the testis in mice and humans, consisting of tissues as diverse as hair, muscle, bone and even complete teeth as well as a stem cell population.
Teratocarcinomas also containing stem cells or embryonal carcinoma (EC) cells were found to be induced in mice by transferring embryos to extrauterine sites. EC cells could be isolated and grown in culture without losing the capacity to differentiate. This was most strikingly demonstrated by introducing them into embryos where they were able to form chimaeras and contribute to all somatic tissues. These studies were followed by attempts to isolate stem cells directly from mouse embryos, without an intermediate teratocarcinoma stage. In 1981, two groups succeeded in establishing mouse ESC lines [25, 26]. In view of the similarities between mouse and human teratocarcinomas and their spontaneous occurrence in the testis, it was predicted that ESCs could be isolated from human embryos. The motivation initially was for studying early human development, but later perspectives for cell transplantation therapies became evident. In 1998 the first HESCs were derived from blastocysts surplus to requirements for assisted reproduction. The markers developed by pathologists to diagnose EC cells in human tumours provided the first evidence of their undifferentiated phenotype; their capacity to form teratocarcinomas containing many tissue types in immunodeficient mice confirmed their pluripotency [27].
A second group described the isolation of two HESC lines independently soon after [28]. Since then, almost 400 HESC lines have been derived worldwide, many of which are now being collectively characterized in a large international consortium [29]. In addition, many publications have described their differentiation to various cell types in culture in response to cytokines, hormones and growth conditions. These include neural cells (neurons, glia and oligodendrocytes), vascular endothelial cells, insulin-producing pancreas cells, cartilage and bone, cardiomyocytes, hematopoietic cells and hepatocytes (reviewed in [30]).
HESC differentiation to cardiomyocytes
The first report of cardiomyocyte differentiation [31] appeared almost 3 years after HESCs were first derived. To induce cardiomyogenesis, cells were dispersed into small clumps of 3–20 cells and grown for 7–10 days in suspension to form structures like embryoid bodies (EBs) from mESCs. This approach was based on that developed in the 1990s for mESCs by the groups of Doetschman and Wobus (reviewed in [4]). After plating onto culture dishes, beating areas were observed in ∼8% of the outgrowths 20 days later. This spontaneous differentiation to cardiomyocytes in HESC aggregates was also observed by others [32], but in this case approximately 25% of the EBs were beating after 8 days of differentiation and 70% after 20 days. Other reports described spontaneous differentiation of cardiomyocytes from HESCs, with 10–25% of the embryoid bodies beating after several weeks [33]. The reasons for these differences in efficiency are not clear, but cell lines appear to differ and counting beating EBs may not accurately reflect the conversion of HESC to cardiomyocytes; variable numbers of cardiac cells and non-cardiomyocytes may be present. An alternative differentiation method is based on co-culture of HESC with a visceral endoderm-like cell line (END-2) or growth of HESC EBs in END-2 conditioned medium [34, 35]. Since (visceral) endoderm plays an important role in the differentiation of cardiogenic precursor cells in the adjacent mesoderm in vivo during development, the underlying molecular mechanism may reflect that occurring in the embryo. All of these methods result in conversion of HESCs to cardiomyocytes at relatively low efficiencies however, illustrating the possible benefits to be derived from a better understanding of the stepwise process of cardiac development.
Molecular control of cardiac development
The process of forming a heart in a developing embryo requires many signals, some of which originate outside the pre-cardiac mesoderm and some of which originate in the developing heart. The fruitfly Drosophila melanogaster has been a major source of insights into the molecular control of heart development. Three main families of peptide growth factors have thus been identified as being essential for heart development, and all have proved to be of similar importance in heart development in mammals, both as positive and negative regulators. These are the bone morphogenetic proteins (BMPs), members of the transforming growth factor β superfamily, the Wnts and the fibroblast growth factors (FGFs). Members of all of these families or their inhibitors are expressed in endoderm. Disrupted expression of these ligands, receptors or their downstream target genes has dramatic and distinct effects on cardiac development that are highly conserved between species (reviewed in [36]). BMPs control several major cardiac specific transcription factors, including Nkx 2-5, the mammalian homologue of tinman, through SMAD binding sites [16, 37, 38]. BMP2, 4 and 7 are co-expressed spatially and temporally with GATA-4 and Nkx 2-5 in the pre-cardiac mesoderm, again suggesting they may control the expression of cardiac transcription factors [39, 40]. As in Drosophila, treatment of mammalian embryos with BMP results in the ectopic expression of Nkx 2-5 and GATA-4 [39]. The addition of noggin, a BMP antagonist, to developing embryos inhibits differentiation of cardiac cells [39, 41]. Mouse BMP2−/− mutants have abnormal heart development, but heart precursors develop normally, suggesting that BMP2 is not required for the induction of cardiomyocytes, but for their subsequent organization [42]. BMP2 is also expressed in endoderm, a tissue adjacent to the heart-forming region and containing the most cardiac inductive activity [39]. BMP5 and 7 double knockout mice have severely delayed cardiac morphogenesis [43]. In general, therefore, BMP signaling appears to promote cardiogenesis in vertebrates [39, 44–48] and is also required to generate mesoderm/cardiac muscle cells from mouse EC cells and ESCs in culture [49].
Wingless in Drosophila and related Wnt proteins in vertebrates are involved in cardiac specification, although their function in mammals is complex. Wnts were initially considered suppressive of heart formation, but both induction and inhibition have since been reported. The ‘canonical’ Wnts 1, 3A and 8, acting by inhibition of GSK3 allowing nuclear localization of β-catenin, appear to inhibit cardiac differentiation, whereas the non-canonical Wnt 11, involving protein kinase C, seems to enhance cardiac differentiation (reviewed in [36]). Supporting this, inhibition of the canonical Wnt signaling increases cardiac differentiation [50], and conditional deletion of β-catenin from the definitive endoderm of the mouse results in the formation of multiple ectopic hearts [51]. The presence of crescent, dkk-1 or other Wnt antagonists induces cardiomyocyte differentiation in non-heart-producing mesoderm [50, 52, 53]. Wnts 3A and 8 block Nkx 2-5 and Tbx expression and therefore cardiomyocyte differentiation [50]. However, in contrast to these findings Wnt3A and Wnt8 were found to promote cardiac differentiation in P19Cl6 cells, a clonal line derived form P19 EC cells [54]. The complexity of this matter is discussed in detail by Olson and Schneider [36]. Recent findings showing that β-catenin signaling must be blocked for heart valve formation in zebrafish also demonstrate a negative role for Wnts in the development of the heart [55]. We recently observed a similar negative effect of canonical Wnt-signalling on cardiac differentiation in the HESC-END-2 co-culture system. BIO, a small molecular activator of canonical Wnt signaling, inhibited not only the number of beating aggregates that form in the cultures but also reduced cardiac marker expression at the protein and RNA levels (Fig. 2).

Pharmacological GSK-3 inhibitor BIO activates Wnt signalling and blocks cardiac differentiation of HESCs. To induce cardiac differentiation, HES2 cells were co-cultured with END2 feeders [35] and cultured in a serum-free medium for at least 12 days [108]. At day 5, the medium was changed, and BIO was added at a concentration of 1 or 2 µM in serum-free medium (or serum-free medium only, for control). At day 9 and 12, the co-cultures were refreshed with serum-free medium only, then harvested for RNA or protein isolation. (a) Scoring of the number of areas of beating muscle in the co-cultures at day 12 showed that BIO was inhibitory. On average, the reduction in the number of beating areas was 18-fold in the presence of 1 µM BIO and 61-fold in the presence of 2 µM BIO, respectively, compared with control values. (b) Determining the expression of two cardiac proteins, α-actinin and βMHC, by real-time polymerase chain reaction (PCR) showed a reduction in the presence of BIO addition by 10- and 11- fold, respectively, in the presence of 1 µM BIO and 164- and 93-fold, respectively, in the presence of 2 µM BIO. The cycle number at which the reaction crossed an arbitrary threshold (Ct) was determined for each gene. The relative number of messenger RNA levels was determined by 2-DCt. Relative gene expression was normalized to hARP expression. (c) Analysis of the effect of BIO on cardiac differentiation in 17-day co-cultures by Western blotting showed a strong decrease in the expression of the cardiac marker tropomyosin in the presence of BIO. p values were determined using the Man-Whitney test.
Wnt 11, a non-canonical Wnt, can by contrast induce cardiomyogenesis in the non-precardiac mesoderm of chick embryos [56]. This may be a result of its ability to block canonical Wnt signaling by sequestering cytoplasmic β-catenin and inducing cardiomyogenesis. Results have not yet been reconciled but may relate to distinct effects of the canonical (acting via β-catenin/GSK3 to repress cardiogenesis) versus non-canonical (acting via PKC/JNK to promote cardio-genesis) signaling pathways, and/or indirect effects in certain model systems (e.g., induction, expansion or augmentation of BMP-producing endoderm-like cells). The state of the cells at the time of receiving the signal combined with the presence of specific cofactors may determine the ultimate biological response.
Finally, some limited studies in chick and zebrafish have implicated a cardioinductive role for FGFs [57–59], although in Drosophila, the functions of FGFs in heart development have been investigated in more detail because of the availability of specific mutants. Drosophila has only two FGF receptors, and only one of them, heartless (htl), is expressed in the mesoderm in early gastrulation and during differentiation; it is required for normal cardiac development [60–62]. Htl mutants have no dorsal vessel, the cardiac organ in Drosophila [60]. This is probably due in part to a role in directing the migration of cardiac precursors in the mesoderm (reviewed in [60]). However, in addition to the ability of htl to direct migration, it also plays a direct role in cardiomyogenic specification; blocking htl function after migration has occurred also blocks cardiac precursor specification [62].
There are multiple FGF family members in vertebrates, although not all have been implicated in heart development. FGFs 1, 2 and 4 have been identified as being secreted by the portion of the developing embryo that is necessary for cardiac development, although their exact role is unclear. What is clear is that they cooperate with BMPs to induce cardiomyogenesis [58]. In chick embryos, FGF2 and 4 induce cardiomyogenesis in non-precardiac mesoderm, but the differentiation is much more efficient if BMP2 or 4 is also present [58, 63]. Another family member, FGF8, is expressed in the cardiac mesoderm of mice, chicks and zebrafish [59, 64, 65]. Again, BMPs seem to cooperate with FGF8 in heart induction and morphogenesis, BMP2 upregulating FGF8 in chick embryos [59] and synergizing to drive mesodermal cells into myocardial differentiation. Zebrafish with FGF8 mutations do not express Nkx 2-5 or GATA-4 in the precardiac mesoderm and have severely deformed ventricles [65]. This may be directly or indirectly due to the fact that these mutant zebrafish have less Nkx 2-5 and GATA-4 expression [65]. These three signalling pathways activated by BMP, Wnt and FGF ligands are essential not only for primary cardiogenesis but are also involved in secondary (AHF) cardiogenesis (reviewed in [16]).
Once anterior mesoderm cells have received appropriate signals, such as those described above, they switch on a set of cardiac-restricted transcription factors that interact in combination to control downstream genes in the cardiac pathway. The homeodomain transcription factor Nkx2.5 [66] and the T-box protein Tbx5 [67, 68] are among the earliest markers of the cardiac lineage and are activated shortly after cells have formed the heart fields. Nkx2.5 is thought to be required in mice specifically for left ventricular chamber development [69], whilst loss of Tbx5 results in severe hypoplasia of both the atrial and left ventricular compartments [70] and may thus be important for the formation of both. Nkx2.5 and Tbx5 associate with members of the GATA family of zinc finger transcription factors and with serum response factor (SRF) to activate cardiac structural genes such as actin, myosin light chain (MLC), myosin heavy chain (MHC), troponins and desmin. Tbx5 can also cooperate with Nkx2.5 to activate expression of ANF and the junctional protein connexin 40 [70, 71]. Members of the myocyte enhancer factor 2 (MEF2) family of transcription factors also play key roles in cardiomyocyte differentiation by switching on cardiac muscle structural genes. In addition, association of SRF with a nuclear protein myocardin activates cardiac specific promoters [72]. Thus multiple complex interactions take place between various transcription factors to control initial differentiation and maturation of cardiomyocytes. Apart from their functional role, many of these factors serve as excellent markers of cardiomyocytes in differentiating cultures of hESC and mES cells and can be useful in identifying the degree of maturity of specific cardiac cells and the kinetics with which differentiation is taking place because their normal expression is under tight temporal control. A recent addition to this list is Isl1, a LIM homeodomain transcription factor, which identifies a cardiac progenitor population, including cells of the anterior heart field, that proliferates prior to differentiation and contributes the majority of cells to the heart [14]. Unlike skeletal muscle cells, where differentiation and proliferation are mutually exclusive, embryonic cardiomyocytes differentiate and assemble sarcomeres even while they proliferate, although organization is much greater postnatally. The prospect of using Isl1 as a marker for the undifferentiated cardiac progenitor state is exciting, and cell sorting of differentiating hESC on the basis of Isl1 expression could allow further characterization and expansion in culture [3]. This could provide a very useful contribution to upscaling cardiomyocyte production for transplantation.
Characteristics of ESC-derived cardiomyocytes
Fetal, neonatal, mouse ESC(mESC)-derived cardiomyocytes and skeletal myoblasts have been shown to engraft in the myocardium (reviewed in [73]), although in the case of mESC-derived cardiomyocytes, survival after transplantation to an infarcted mouse heart has been problematic [74]. Thus, although functional cardiomyocytes can easily be identified in vitro by their beating phenotype, only more detailed interrogation can establish the identity of the specific cardiac cell types generated, their degree of maturity compared with cardiomyocytes developing in vivo and whether they possess fully functional excitation-contraction coupling machinery that responds appropriately to pharmacological agents.
As discussed earlier, differentiation of human HESCs to the cardiac lineage creates a characteristic gene expression profile [75] reminiscent of both mESC differentiation and the early stages of normal mouse heart development [76]. Analysis of RNA and proteins from HESC-derived cardiomyocytes (HESC-CMs) has demonstrated the presence of cardiac transcription factors, including GATA-4, myocyte enhancer factor (MEF-2) and Nkx2 transcription factor-related locus 5 (Nkx2.5) [31, 32].
Correspondingly, structural components of the myofibers are appropriately expressed. These include α-, β- and sarcomeric-myosin heavy chain (MHC), atrial and ventricular forms of myosin light chain (MLC-2a and -2v), tropomyosin, α-actinin and desmin, although in contrast to mouse, heart chamber-restricted expression of structural proteins is less well defined in human heart, MLC-2v, for example, is restricted to the ventricle in mouse and human fetal hearts but MLC-2a is expressed in both atrium and ventricle in humans and not just in atria as in mice [77]. This implies that using protein or gene expression profiles to determine the phenotype of HESC-CMs in culture should be done with caution. Antibody reactivity to two members of the troponin complex, cardiac troponin T (cTnT), which binds to tropomyosin, and cardiac troponin I (cTnI), which provides a calcium-sensitive molecular switch for regulation of striated muscle contraction, has been demonstrated. cTnI appears to be truly cardiac specific, as antibodies to this protein only react with cells arising from beating and not non-beating regions. In addition, upregulation of atrial natriuretic factor (ANF), a hormone expressed in both atrial and ventricular cardiomyocytes in the developing heart, has also been observed during cardiac differentiation of HESCs. Moreover, these cells express creatine kinase-MB (CK-MB) and myoglobin [32]. Thus, many of the transcription factors, structural proteins and metabolic regulators of cardiac development are found within HESC-CMs, although they also react with antibodies to smooth muscle actin, a protein found in embryonic and fetal, but not adult cardiomyocytes, suggesting a limited degree of maturation [32]. Single HESC cardiomyocytes display various morphologies in culture and may be spindle-shaped, round, tri- or multi-angular, rather than the rod shape of mature cells; sarcomeric immunostaining shows striations in separated bundles, rather than the highly organized parallel bundles, as in human adult cardiomyocytes; and the action potentials determined by patch-clamp electrophysiology show ventricular phenotypes with upstroke velocities ∼10 times lower than those of adult cardiomyocytes [33, 35]. It is of interest to note that not only are HESC-CMs connected to each other by connexin-43 expressing gap junctions [33], they are also capable of forming de novo gap junctions with primary human cardiomyocytes. In HESC-CMs co-cultured with primary human fetal cardiomyocytes, injection of the dye ‘Lucifer Yellow’ into the HESC-CMs results in rapid transfer of the dye via gap junctions, into the underlying primary cardiomyocytes [78]. This ability to couple with primary cardiomyocytes was not observed in skeletal myoblasts. Despite their immaturity, HESC-CMs may be useful in understanding the activity of some pharmacological agents in (adult) human cardiomyocytes, e.g. the L-type Ca2+ channel is inhibited by verapramil, indicating that it is already coupled to downstream signalling pathways, as in postnatal cardiomyocytes but in contrast to mESC-CM.
Because of their immaturity, they may be an excellent source of cells for transplantation in terms of their ability to survive and integrate [79, 80], and maturation may take place in situ in the heart. For other purposes, such as the studying the physiological changes associated with genetic or degenerative disease in the adult heart, mature human cardiomyocytes may be required. Among the possibilities for achieving this in culture is prolonged culture or cyclic stretch or electrical stimulation. HESCs can provide useful information on the molecular mechanisms controlling early differentiation in the human heart. Analysis of gene expression by microarray during HESC-CM differentiation [75] showed that apart from identifying most known cardiac transcription factors, such as MEF2C, TBX2 and TBX5 and genes encoding structural proteins, we observed upregulation of multiple known genes not previously associated with cardiac development and several unexpected genes enriched or even uniquely expressed in the heart. Some of these are conserved across species and show restricted expression patterns in both mouse and human fetal heart; further analysis by deletion in the mouse should shed light on the function for these genes, not only in mice but also in relation to congenital heart defects in humans. This reflects a more general strategy using HESCs for functional analysis and gene mining in human development.
Resident cardiac stem cells and ‘bar codes’ for the mesoderm and cardiac lineage
It is clear that establishing the molecular identity of the cellular intermediates and the signalling receptors they express would also contribute towards optimizing each of the individual differentiation events and therefore to the overall efficiency of converting stem or progenitor cells into cardiomyocytes. This is of particular relevance when adding growth factors or small molecular agonists or antagonists to the specific pathways now identified as being important in heart development and specification. Several studies in mESCs have now used particular cell surface proteins and transcription factors as markers to separate cells with different phenotypes at selected, early stages of differentiation. This appears to facilitate enrichment for particular cell types and has been most effectively used for the mesodermal lineage, which gives rise to most cardiovascular cell types. Applying similar approaches to HESCs could result in significant improvements in the efficiency of stem cell to cardiomyocyte conversion. It is possible that the transient cardiac progenitor stage through which ESCs pass during differentiation to cardiomyocytes is similar to that of resident CPCs or CSCs in the fetal or adult heart, although the distinction between CPCs and CSCs is not entirely clear. They may represent different stages of the same type of cell or be subsets of a more broadly defined cell population in the heart (reviewed in [6]). They have often been selected on the basis of general features of stem cells from other tissues, such as cell surface markers or specific biochemical properties, for example, the ability to efflux Hoechst dye [81]. Cell surface markers, however, are of particular interest since fluorescent or magnetic sorting based on a cell surface antibody binding would be useful for selecting CPCs/CSCs or cardiomyocytes for transplantation from primary tissue or possibly differentiating HESC cultures. Although few suitable cell surface protein-antibody combinations have been identified for these cell types, their potential usefulness in enriching mixed cell populations for particular cell subsets is becoming clear. In the following section, cell surface proteins are discussed in the context of analysis of gene function in heart development in mice.
Cell surface proteins and the isolation of progenitor cells from the heart or ESCs
The generation of cell subpopulations with cardiac differentiation potential has largely been based on segregating cells which express receptors thought to be involved in promoting the cardiogenic lineage within the embryo.
Extracellular signalling molecules pivotal to cardiac development were exemplified by gene knockout and conditional targeting of genes in mice. Developmental cardiac phenotypes were observed in myocardial specific knockouts of the receptor binding signalling molecule for vascular endothelial growth factor (VEGF), Vegfa, the BMP receptor Bmpr1a (or ALK3) and the FGF receptors Fgfr1/Fgfr2. The cardiomyocyte specific deletion of Fgfr1/Fgfr2 and the global deletion of its ligand Fgf9 result in reduced cardiac myocyte proliferation and abnormal myocardial development. These findings indicate a role for FGFs in maintaining the cell cycle progression of the cardiomyocyte population in the developing heart. The cardiomyocyte-restricted knockout of Vegfa results in coronary vascular deficiency and myocardial thinning [82–84]. This suggests that the initiation of myocardial compact zone thickening and the development of coronary vasculature, two processes that begin at E11–12 of mouse development, occur in a coupled manner and may involve VEGF-A signalling [85], although this has not been shown directly. There is, however, clearly an interaction between the epicardial and myocardial cells.
Lineage tracing studies in the mouse show that the endocardium and a myocardial cell subpopulation develop from a common lineage precursor that expresses the VEGF-A ligand binding receptor, Flk-1. Also termed VEGFR-2 (vascular endothelial growth factor receptor-2), this is the major signalling receptor for VEGF-A. Flk-1 was shown to be essential for the development of the vascular and hematopoietic lineages in the early embryo and to control blood vessel formation [86, 87].
Unlike hematopoietic differentiation in the mESC cell system, little progress has been made in identifying and characterizing early-stage cardiac progenitors. Using mESCs as a model, Keller and co-workers [89] examined the developmental significance of Flk-1 receptor expression by differentiating the cells as EBs. All cardiac tissue types were thus derived, and gene expression analyses showed that formation of contracting cardiac cells in EBs recapitulates cardiogenesis in the mouse embryo. As early as day 2.5–3.0 EBs contained prehemangioblast mesoderm, evidenced by cells positive for green fluorescent protein (GFP), targeted to the Brachyury (Bry) locus [88, 89]. Brachyury is the founding member of the T box family of transcription factors. It is expressed in all nascent mesoderm and is downregulated as these cells undergo patterning and specification into derivative tissues [90]. Day 3.25 Bry-GFP+ cells from EBs, immunosorted for the presence or absence of Flk-1 receptor, were allowed to reaggregate and attach onto gelatin-coated plates for 3 days. The Flk-1− subpopulation generated adherent clumps which began rhythmically contracting within 2–3 days. The cardiomyocyte phenotype of these cells was confirmed by positive staining with antibodies to troponin-T protein and cardiac transcription factors (Nkx2.5 and cMhc). Immediately after isolation, Flk-1+ cells only expressed hematopoietic transcription factors (Runx1 and Scl) and later markers indicative of maturation along this lineage (Gata-1) [88].
The developmental potential of Bry-GFP+ Flk-1− cells was investigated further by isolating these cells at different stages of EB differentiation. Interestingly, cells from days 2.5 and 3.0 generated a distinct Flk-1 subpopulation expressing high levels of the receptor. Cells isolated from days 3.5 and 4.0 produced fewer Flk-1+ cells expressing low levels of the receptor. Upon reaggregation, day 2.5 and 3.0 cells differentiated robustly towards hematopoietic and vascular cell types. Ten percent of day 3.0 reaggregates also produced beating cardiomyocytes, and this increased to 50% from cells isolated at day 3.5. None of the day 4.0 cell aggregates generated beating structures. These data support the interpretation that hemangioblast and cardiomyocyte cell lineages derive from distinct mesodermal cell subpopulations present at different time points of EB maturation. Both subpopulations are marked by the emergence of Flk-1+ cells; the contribution of the Flk-1low cell subpopulation at day 3.0–3.5 to the production of the cardiac lineage from EBs requires further investigation [88]. The potential for cardiac differentiation in cultured EBs appears to be restricted to a narrow time window present for 12–18 hours from day 3.0 after aggregation onwards. The sequential appearance of cells with hemangioblast and cardiac fates within EBs in a defined kinetic pattern recapitulates the temporal specification of these populations in vivo [91]. Furthermore, the EB environment was shown to inhibit the maturation of cardiac progenitors present at day 3.5 since the plating of unsorted cells generated less than 1% beating cardiomyocytes [88]. The above observations highlight the importance of isolating specific progenitor subpopulations from EB cultures on the basis of intracellular and/or cell surface markers at early stages of differentiation to maximize cardiac cell differentiation (Fig. 1).
The appearance of a mESC-derived subpopulation, positive for Flk-1 which differentiates into beating cardiomyocytes, was also reported using a 2D culture system [92–94]. Here, ESCs were plated onto type IV collagen-coated dishes in the absence of leukemia inhibitory factor (LIF) to allow differentiation. Ninety-six to 108 h later Flk-1+ cells that had developed were purified by flow cytometric sorting and cultured on a monolayer of OP9 stroma cells, a cell line established from the calvaria of op/op mice. This resulted in spontaneous beating of isolated Flk-1+ cells. Neither paraformaldehyde-fixed OP9 cells nor their conditioned medium induced beating, indicating that direct contact was required for cardiomyocyte differentiation. Like the END-2 visceral endoderm-like cells discussed above, which effectively promote cardiac differentiation of some HESC lines, the OP9 cells may provide signals similar to endoderm underlying cardiac mesoderm that is critical for the formation of cardiac cells in the embryo [94].
The isolated Flk-1+ cell subpopulation differentiated into beating cells within 4–5 days of culture on OP9 stroma cells, while Flk-1− cells required a minimum of 8 days to become cardiomyocytes. Using a similar protocol on mESCs expressing a cardiac specific alpha myosin heavy chain (αMHC) promoter-driven GFP produced approximately 10–18% GFP+ cardiomyocytes and outperformed the EB differentiation system by 2–3-fold in the production of contracting cells. The authors further showed that single Flk-1+ cells, plated onto OP9 feeder monolayers, gave rise to heterogeneous cell colonies composed of either endothelial cells only (40% of colonies), a mixture of endothelial and cardiac cells (43% of colonies) or only cardiac cells (16% of colonies). This suggested that Flk-1+ cells are able to develop into cardiomyocytes and endothelial cells at the single cell level. A number of cell surface markers were tested in conjunction with Flk-1+ to derive the progenitor sub-population capable of producing more homogeneous cardiac cell clusters. Cells that co-expressed markers like c-kit and Sca-1 or mesenchymal stem cell markers such as CD44 and CD90 with Flk-1 were examined for their differentiation potential. Either no significant cardiomyocyte differentiation was observed from double positive sub-populations, as in the case of Sca-1/Flk-1 and CD90/Flk-1 cells, or marker expression was unable to identify cardiac-restricted cells as in the case of (c-kit/Flk-1). Interestingly, the unique combination of Flk-1 and CXCR4, a 7-transmembrane spanning G protein-coupled receptor for chemokine CXC12 or SDF-1, produced highly enriched cardiomyocyte colonies which ceased to express either marker upon differentiation. CXCR4 is expressed in splanchnopleuric mesoderm and mesenchymal cells, but not in developing heart cells at E8.5 of mouse development. Flk-1 and CXCR4 were expressed in immature cells that retained cardiogenic potential at the single cell level but were lost in differentiated cardiac cells (Fig. 1) [94].
Aside from mESC cardiac differentiation, which appears to highlight differences between temporally distinct cell subpopulations with or without Flk-1 expression, a range of somatic cells such as bone marrow cells and more recently CPCs and CSCs from cardiac tissues have also been highlighted as a potential source of cardiomyocytes with immunogenically distinct cell phenotypes [95]. These include Lin-c-kit+ CD34− CD45− cells, which were shown to be self-renewing, clonogenic, able to produce cardiomyocytes, smooth muscle cells and endothelial cells in vitro and to contribute to regeneration of the infarcted myocardium in animal models. In culture, these cells have some ‘embryonic’ cell features, including a high nuclear-to-cytoplasmic ratio and active proliferation, and they express some cardiac transcription factors. It is unclear whether CSCs selected as the Lin-c-kit+ fraction originate from resident cells established during heart formation or derive from as yet undefined, circulating bone marrow cells [96]. Other cells include the Sca1+ CD31+ c-kit− adult myocardial progenitors, capable of generating cardiomyocytes after injection into a mouse cardiac infarction model [97]. Messina and co-workers [98] reported the formation of cardiospheres from human and mouse heart cells that expressed Sca-1, c-kit, FLK1, CD31 and connexin 43, and this subpopulation appeared to contribute to cardiac repair in infarcted mouse hearts. Also ‘side population’ cells, identified as Sca1+ CD31− and possessing the ability to efflux Hoechst 33342, have been reported to differentiate into cardiomyocytes in vitro, and be self-renewing and clonogenic [99, 100]. Another CD31− population, the mESC-derived FLk1+ CD31− VE-cadherin− cells can form precursors of the cardiac, endothelial as well as hematopoietic lineages [101]. Other markers that were shown to be highly enriched during early cardiac differentiation of mouse P19 EC cells include pleiotrophin and podocalyxin, surface molecules which could be used to select putative cardiogenic precursors [102].
Recent studies have shown progress in producing HESC derived hematopoietic precursors in EBs or by co-culture with the OP9 stromal cells [103–106]. By comparison, reports showing differentiation of hESCs towards the cardiogenic lineage are limited and show variable efficiencies [5, 6].
Using the END-2/HESC co-culture method described earlier, the appearance of beating structures was shown to be substantially improved (by 24-fold) by omission of fetal calf serum from the culture medium, suggesting that calf serum may contain inhibitory factors. An additional 40% increase in the number of beating areas was observed in the presence of ascorbic acid [107], thought to act as a free-radical scavenger, as previously shown in mESCs.
Although this represents an efficient platform to study mesodermal differentiation of HESCs, a heterogeneous mixture of cells likely in different stages of mesodermal commitment always results. With the potential of applying specialized cells to reverse heart disease, the task at hand is to exploit the current differentiation platform and to isolate HESC-derived, lineage-restricted precursors as shown for mESCs. This could also be approached by selecting specific cell subpopulations from the above culture system targeting specific cell surface markers which identify precursor cells with cardiogenic potential. Microarray analysis conducted on mesodermal cell progeny obtained from END-2/HESC co-culture has shown the induction of early embryonic genes involved in mesoderm specification, like Brachyury T [75], and indicates the presence of mesodermal precursor cell subpopulations like those found in differentiating mESCs. Hence, flow cytometric sorting (FACS) and/or magnetic assisted cell separation (MACS) of differentiating HESCs based on immunogenic profiles of cells found in differentiating mouse ESCs offers the exciting prospect of identifying ESC-derived cardiac precursor cells for selected expansion and production upscale in culture. The purification of these cells currently aims to generate more defined approaches to study cardiac differentiation from HESCs.
Conclusions and perspectives
It is clear that ESCs from both mouse and humans differentiate towards cardiomyocytes that appropriately respond to different pharmacologic stimuli, and this infers functional expression of many of the components required for excitation coupling. However, while maturation of HESC-CMs does occur during prolonged culture, currently these cells fail to attain the characteristic of adult cardiomyocytes. This is likely to benefit attempts to use them for transplantation. However, it will be important to assess novel methods to stimulate maturation so in vitro produced cardiomyocytes with embryonic or adult characteristics are at the disposal of the scientific, clinical and pharmacological community, as this would be potentially useful in drug discovery and testing. In addition, it might be possible to use HESCs to develop in vitro models for studying specific genetic cardiac diseases, such as channelopathies where specific ion channel mutations may cause fatal arrythmias in asymptotic carriers or to use them to identify the function of genes associated with congenital heart defects. HESCs and mESCs recapitulate the differentiation of cardiac cells in the development of humans and mice respectively, both in terms of gene and protein expression as well as physiological function. They thus provide a unique opportunity to study heart development at stages where, at least in humans, the heart is not accessible. In turn, this may allow functional analysis of developmental genes in vitro which may provide new clues into the genetic basis of congenital heart defects in humans. Gene sequencing technology is now so advanced and rapid that it is little problem to interrogate several hundred genomes in a short time for mutations in selected genes. This may yield new screens for prenatal genetic diagnosis in humans and prevent the birth of children with congenital heart defects.
In terms of transplantation, it is also important to be aware that whilst introduction of ectopic cardiac cells in mice might not cause arrythmias because of the high heart rate and adaptive capacity of the mouse heart, this may not be the case in humans. Transplantation of skeletal myoblasts in patients has already caused serious clinical complications [108, 109] because of inadequate incorporation into the host myocardium. More recently, transplantation of HESC-derived cardiomyocytes into the hearts of pigs was described [110]. Since pig heart physiology is more reminiscent of human heart than rodents, the observation of ectopic pacemaker-like activity from the transplanted cells cautions against premature clinical application. There are few proven sources of bone fide cardiomyocytes in humans, but to date HESC-derived cardiomyocytes and cardiac progenitor cells appear to be retaining a status of clinical potential.
From an optimistic perspective, the development of techniques for somatic cell reprogramming, perhaps cloning, to derive stem cells from a patient’s own tissue may ultimately eliminate the use of immunosuppressive therapy in cell transplantation. The use of HESC-derived cardiomyocytes for transplantation, however, ultimately requires that the population be devoid of non-cardiac cells to obtain optimal engraftment and shows no evidence of contamination with undifferentiated stem cells that could cause teratomas in vivo. From a societal stance, ischemic heart disease and related pathologies are the most prevalent consequences of mortality in the Western world. While pharmacological therapy for patients improves cardiac function, survival and quality of life, the natural course of the disease cannot be halted, and gradual progress towards severely impaired cardiac function and death is generally inevitable. If it were possible to reconstitute the heart by replacing poorly contracting cells and scarred, post-ischemic tissue with functional HESC-derived precursors to remodel the myocardium, these problems could be circumvented.
References
Beltrami, A.P., Torella, D., Baker, M., Limana, F., Chimenti, S., Kasahara, H., Rota, M., Musso, E., Urbanek, K., Leri, A., Kajstura, J. et al. (2003) Adult cardiac stem cells are multipotent and support myocardial regeneration. Cell 114, 763–776.
Urbanek, K., Cesselli, D., Rota, M., Nascimbene, A., De Angelis, A., Hosoda, T., Bearzi, C., Boni, A., Bolli, R., Kajstura, J et al. (2006) Stem cell niches in the adult mouse heart. Poc. Natl. Acad. Sci. USA 103, 9226–9231.
Laugwitz, K. L., Moretti, A., Lam, J., Gruber, P., Chen, Y., Woodard, S., Lin, L. Z., Cai, C. L., Lu, M. M., Reth, M., Platoshyn, O., Yuan, J. X., Evans, S. and Chien, K. R. (2005) Postnatal isl1+ cardioblasts enter fully differentiated cardiomyocyte lineages. Nature 433, 647–653.
Passier, R. and Mummery, C. (2003) Origin and use of embryonic and adult stem cells in differentiation and tissue repair. Cardiovasc. Res. 58, 324–335.
Passier, R. and Mummery, C. (2005) Cardiomyocyte differentiation from embryonic and adult stem cells. Curr. Opin. Biotechnol. 16, 498–502.
van Laake, L. W., Van Hoof, D. and Mummery, C. L. (2005) Cardiomyocytes derived from stem cells. Ann. Med. 37, 499–512.
Reinecke, H., Zhang, M., Bartosek, T. and Murry, C.E. (1999) Survival, integration, and differentiation of cardiomyocyte grafts: a study in normal and injured rat hearts. Circulation. 100, 193–202.
Leobon, B., Garcin, I., Menasche, P., Vilquin, J.T., Audinat, E. and Charpak, S. (2003) Myoblasts transplanted into rat infarcted myocardium are functionally isolated from their host. Proc. Natl. Acad. Sci. USA 100, 7808–7811.
Soonpaa, M. H., Koh, G.Y., Klug, M.G. and Field, L. J. (1994) Formation of nascent intercalated disks between grafted fetal cardiomyocytes and host myocardium. Science 264, 98–101.
Leor, J., Patterson, M., Quinones, M. J., Kedes, L. H. and Kloner, R. A. (1996) Transplantation of fetal myocardial tissue into the infarcted myocardium of rat. A potential method for repair of infarcted myocardium? Circulation 94(9 Suppl.), II332–II336.
Stoffel, M., Vallier, L. and Pedersen, R. A. (2004) Navigating the pathway from embryonic stem cells to beta cells. Semin. Cell. Dev. Biol. 15, 327–336.
Wichterle, H., Lieberam, I., Porter, J.A. and Jessell, T. M. (2002) Directed differentiation of embryonic stem cells into motor neurons. Cell 110, 385–397.
Garcia-Martinez, V. and Schoenwolf, G. C. (1993) Primitive-streak origin of the cardiovascular system in avian embryos. Dev. Biol. 159, 706–719.
Olson, E. N. Development. (2001) The path to the heart and the road not taken. Science. 291, 2327–2328.
Brand, T. (2003) Heart development: molecular insights into cardiac specification and early morphogenesis. Dev. Biol. 258, 1–19.
Nascone, N. and Mercola, M. (1995) An inductive role for the endoderm in Xenopus cardiogenesis. Development 121, 515–523.
Schultheiss, T. M., Xydas, S., and Lassar, A. B. (1995) Induction of avian cardiac myogenesis by anterior endoderm. Development 121, 4203–4214.
Molkentin, J. D., Lin, Q., Duncan, S. A. and Olson, E. N. (1997) Requirement of the transcription factor GATA4 for heart tube formation and ventral morphogenesis. Genes. Dev. 11, 1061–1072.
Roebroek, A. J., Umans, L., Pauli, I.G., Robertson, E. J., van Leuven, F., Van de Ven, W. J. and Constam, D. B. (1998) Failure of ventral closure and axial rotation in embryos lacking the proprotein convertase Furin. Development 125, 4863–4876.
Saga, Y., Miyagawa-Tomita, S., Takagi, A., Kitajima, S., Miyazaki, J., and Inoue, T. (1999) MesP1 is expressed in the heart precursor cells and required for the formation of a single heart tube. Development 126, 3437–3447.
Reiter, J. F., Alexander, J., Rodaway, A., Yelon, D., Patient, R., Holder, N. and Stainier, D. Y. (1999) Gata5 is required for the development of the heart and endoderm in zebrafish. Genes Dev. 13, 2983–2995.
Kelly, R.G. and Buckingham, M.E. (2002) The anterior heart-forming field: voyage to the arterial pole of the heart. Trends. Genet. 18, 210–216.
Christoffels, V. M., Habets, P. E., Franco, D., Campione, M., de Jong, F., Lamers, W. H., Bao, Z. Z., Palmer, S., Biben, C., Harvey, R. P et al. (2000) Chamber formation and morphogenesis in the developing mammalian heart. Dev. Biol. 223, 266–278.
Evans, M. J. and Kaufman, M. H. (1981) Establishment in culture of pluripotential cells from mouse embryos. Nature. 292, 154–156.
Martin, G. R. (1981) Isolation of a pluripotent cell line from early mouse embryos cultured in medium conditioned by teratocarcinoma stem cells. Proc. Natl. Acad. Sci. USA 78, 7634–7638.
Thomson, J. A., Itskovitz-Eldor, J., Shapiro, S. S., Waknitz, M. A, Swiergiel, J. J., Marshall, V. S., and Jones, J. M. (1998) Embryonic stem cell lines derived from human blastocysts. Science 282, 1145–1147.
Reubinoff, B.E., Pera, M.F., Fong, C.Y., Trounson, A. and Bongso, A. (2000) Embryonic stem cell lines from human blastocysts: somatic differentiation in vitro. Nat. Biotechnol. 18, 399–404.
Andrews, P. W., Benvenisty, N., McKay, R., Pera, M. F., Rossant, J., Semb, H. and Stacey, G. N. (2005) The International Stem Cell Initiative: toward benchmarks for human embryonic stem cell research. Nat Biotechnol. 23, 795–797.
Pera, M. F. and Trounson, A. O. (2004) Human embryonic stem cells: prospects for development. Development. 131, 5515–5525.
Kehat, I., Kenyagin-Karsenti, D., Snir, M., Segev, H., Amit, M., Gepstein, A., Livne, E., Binah, O., Itskovitz-Eldor, J., and Gepstein, L. (2001) Human embryonic stem cells can differentiate into myocytes with structural and functional properties of cardiomyocytes. J. Clin. Invest. 108, 407–414.
Xu, C., Police, S., Rao, N. and Carpenter, M.K. (2002) Characterization and enrichment of cardiomyocytes derived from human embryonic stem cells. Circ. Res. 91, 501–508.
He, J.Q., Ma, Y., Lee,, Y., Thomson, J.A. and Kamp, T.J. (2003) Human embryonic stem cells develop into multiple types of cardiac myocytes: action potential characterization. Circ. Res. 93, 32–39.
Mummery, C., Ward, D., van den Brink, C. E., Bird, S. D., Doevendans, P. A., Opthof, T., Brutel de la Riviere, A., Tertoolen, L., van der Heyden, M., and Pera, M. (2002) Cardiomyocyte differentiation of mouse and human embryonic stem cells. J. Anat. 200, 233–242.
Mummery, C., Ward-van Oostwaard, D., Doevendans, P., Spijker, R., van den Brink, S., Hassink, R., van der Heyden, M., Opthof, T., Pera, M., de la Riviere, A. B., Passier, R., and Tertoolen, L. (2003) Differentiation of human embryonic stem cells to cardiomyocytes: role of coculture with visceral endoderm-like cells. Circulation 107, 2733–2740.
Olson, E. N. and Schneider, M. D. (2003) Sizing up the heart: development redux in disease. Genes. Dev. 17, 1937–1956.
Liberatore, C. M., Searcy-Schrick, R. D., Vincent, E. B. and Yutzey, K. E. (2002) Nkx-2.5 gene induction in mice is mediated by a Smad consensus regulatory region. Dev. Biol. 244, 243–256.
Lien, C. L., McAnally, J., Richardson, J. A. and Olson, E. N. (2002) Cardiac-specific activity of an Nkx2-5 enhancer requires an evolutionarily conserved Smad binding site. Dev. Biol. 244, 257–266.
Schultheiss, T.M., Burch, J. B. and Lassar, A. B. (1997) Arole for bone morphogenetic proteins in the induction of cardiac myogenesis. Genes. Dev. 11, 451–462.
Andree, B., Duprez, D., Vorbusch, B., Arnold, H. H. and Brand, T. (1998) BMP-2 induces ectopic expression of cardiac lineage markers and interferes with somite formation in chicken embryos. Mech. Dev. 70, 119–131.
Schlange, T., Andree, B., Arnold, H. H., and Brand, T. (2000) BMP2 is required for early heart development during a distinct time period. Mech.Dev. 91, 259–270.
Zhang, H. and Bradley, A. (1996) Mice deficient for BMP2 are nonviable and have defects in amnion/chorion and cardiac development. Development 122, 2977–2986.
Solloway, M. J. and Robertson, E. J. (1999) Early embryonic lethality in Bmp5;Bmp7 double mutant mice suggests functional redundancy within the 60A subgroup. Development 126, 1753–1768.
Zaffran, S. and Frasch, M. (2002) Early signals in cardiac development. Circ. Res. 91, 457–469.
Schneider, M. D., Gaussin, V. and Lyons, K. M. (2003) Tempting fate: BMP signals for cardiac morphogenesis. Cytokine Growth Factor Rev. 14, 1–4.
Shi, Y., Katsev, S., Cai, C., and Evans, S. (2000) BMPsignaling is required for heart formation in vertebrates. Dev. Biol. 224, 226–237.
Krishnan, P, King, M. W., Neff, A. W., Sandusky, G. E., Bierman, K. L., Grinnell, B. and Smith, R. C. (2001) Human truncated Smad 6 (Smad 6s) inhibits the BMP pathway in Xenopus laevis. Dev. Growth Differ. 43, 115–132.
Gaussin, V., Van de Putte, T., Mishina, Y., Hanks, M. C., Zwijsen, A., Huylebroeck, D., Behringer, R. R. and Schneider, M. D. (2002) Endocardial cushion and myocardial defects after cardiac myocyte-specific conditional deletion of the bone morphogenetic protein receptor ALK3. Proc. Natl. Acad. Sci.USA 99, 2878–2883.
Johansson, B. M., and Wiles, M. V. (1995) Evidence for involvement of activin A and bone morphogenetic protein 4 in mammalian mesoderm and hematopoietic development. Mol. Cell. Biol. 15, 141–151.
Schneider, V. A. and Mercola, M. (2001) Wnt antagonism initiates cardiogenesis inXenopus laevis. GenesDev. 15, 304–315.
Lickert, H., Kutsch, S., Kanzler, B., Tamai, Y., Taketo, M.M. and Kemler, R. (2002) Formation of multiple hearts in mice following deletion of beta-catenin in the embryonic endoderm. Dev. Cell 3, 171–181.
Marvin, M. J., Di Rocco, G., Gardiner, A., Bush, S. M. and Lassar, A. B. (2001) Inhibition of Wnt activity induces heart formation from posterior mesoderm. Genes Dev. 15, 316–327.
Tzahor E. and Lassar, A. B. (2001) Wnt signals from the neural tube block ectopic cardiogenesis. Genes Dev. 15, 255–260.
Nakamura, T., Sano, M., Songyang, Z., and Schneider, M. D. (2003) A Wnt- and beta -catenin-dependent pathway for mammalian cardiac myogenesis. Proc. Natl. Acad. Sci. USA. 100, 5834–5839.
Hurlstone, A. F., Haramis, A. P., Wienholds, E., Begthel, H., Korving, J., Van Eeden, F., Cuppen, E., Zivkovic, D., Plasterk, R. H. and Clevers, H. (2003) The Wnt/beta-catenin pathway regulates cardiac valve formation. Nature 425, 633–637.
Eisenberg, C. A. and Eisenberg, L. M. (1999) WNT11 promotes cardiac tissue formation of early mesoderm. Dev. Dyn. 216, 45–58.
Lough, J., Barron, M., Brogley, M., Sugi, Y., Bolender, D. L. and Zhu, X. (1996) Combined BMP-2 and FGF-4, but neither factor alone, induces cardiogenesis in non-precardiac embryonic mesoderm. Dev. Biol. 178, 198–202.
Barron, M., Gao, M. and Lough, J. (2000) Requirement for BMP and FGF signaling during cardiogenic induction in nonprecardiac mesoderm is specific, transient, and cooperative. Dev. Dyn. 218, 383–393.
Alsan, B. H. and Schultheiss, T.M. (2002) Regulation of avian cardiogenesis by Fgf8 signaling. Development 129, 1935–1943.
Narasimha, M. and Leptin, M. (2000) Cell movements during gastrulation: come in and be induced. Trends Cell Biol. 10, 169–172.
Gisselbrecht, S., Skeath, J. B., Doe, C. Q., and Michelson, A. M. (1996) Heartless encodes a fibroblast growth factor receptor (DFR1/DFGF-R2) involved in the directional migration of early mesodermal cells in the Drosophila embryo. Genes Dev. 10, 3003–3017.
Michelson, A. M., Gisselbrecht, S., Zhou, Y., Baek, K. H. and Buff, E. M. (1998) Dual functions of the heartless fibroblast growth factor receptor in development of the Drosophila embryonic mesoderm. Dev. Genet. 22, 212–229.
Ladd, A. N., Yatskievych, T. A., and Antin, P. B. (1998) Regulation of avian cardiac myogenesis by activin/TGFbeta and bone morphogenetic proteins. Dev. Biol. 204, 407–419.
Crossley, P. H. and Martin, G. R. (1995) The mouse Fgf8 gene encodes a family of polypeptides and is expressed in regions that direct outgrowth and patterning in the developing embryo. Development 121, 439–451.
Reifers, F., Walsh, E. C., Leger, S., Stainier, D. Y., and Brand, M. (2000) Overlapping and distinct functions provided by fgf17, a new zebrafish member of the Fgf8/17/18 subgroup of Fgfs. Development 127, 225–235.
Lints, T. J., Parsons, L. M., Hartley, L., Lyons, I. and Harvey, R. P. (1993) Nkx-2.5: a novel murine homeobox gene expressed in early heart progenitor cells and their myogenic descendants. Development 119, 969.
Bruneau, B. G., Logan, M., Davis, N., Levi T., Tabin, C. J., Seidman, J. G. and Seidman, C. E. (1999) Chamber-specific cardiac expression of Tbx5 and heart defects in Holt-Oram syndrome. Dev. Biol. 211, 100–108.
Horb, M. E. and Thomsen, G. H. (1999) Tbx5 is essential for heart development. Development 126, 1739–1751.
Yamagishi, H., Yamagishi, C., Nakagawa, O., Harvey, R. P., Olson, E. N. and Srivastava, D. (2001) The combinatorial activities of Nkx2.5 and dHAND are essential for cardiac ventricle formation. Dev. Biol. 239: 190–203.
Bruneau, B. G., Nemer, G., Schmitt, J. P., Charron, F., Robitaille, L., Caron, S., Conner, D. A., Gessler, M., Nemer, M., Seidman, C. E. and Seidman, J.G. (2001) A murine model of Holt-Oram syndrome defines roles of the T-box transcription factor Tbx5 in cardiogenesis and disease. Cell 106, 709–721.
Habets, P. E., Moorman, A. F., Clout, D. E., van Roon, M. A., Lingbeek, M., van Lohuizen, M., Campione, M., and Christoffels, V. M. (2002) Cooperative action of Tbx2 and Nkx2.5 inhibits ANFexpression in the atrioventricular canal: implications for cardiac chamber formation. Genes Dev. 16, 1234–1246.
Wang, D., Chang, P. S., Wang, Z., Sutherland, L., Richardson, J. A., Small, E., Krieg, P. A., and Olson, E. N. (2001) Activation of cardiac gene expression by myocardin, a transcriptional cofactor for serum response factor. Cell 10, 851–862.
Cai, C.L., Liang, X., Shi, Y., Chu, P.H., Pfaff, S. L., Chen, J. and Evans, S. (2003) Isl1 identifies a cardiac progenitor population that proliferates prior to differentiation and contributes a majority of cells to the heart. Dev. Cell 5, 877–889.
Dowell, J.D., Rubart, M., Pasumarthi, K.B., Soonpaa, M.H. and Field, L.J. (2003) Myocyte and myogenic stem cell transplantation in the heart. Cardiovasc. Res. 58, 336–350.
Klug, M.G., Soonpaa, M.H., Koh, G.Y. and Field, L.J. (1996) Genetically selected cardiomyocytes from differentiating embronic stem cells form stable intracardiac grafts. J. Clin. Invest. 98, 216–224.
Beqqali, A., Kloots, J., Ward-van Oostwaard, D., Mummery, C. and Passier, R. (2006) Genome-wide transcriptional profiling of human embryonic stem cells differentiating to cardiomyocytes. Stem Cells 24, 1956–1967.
Fijnvandraat, A. C., van Ginneken, A. C., de Boer, P. A., Ruijter, J. M., Christoffels, V. M., Moorman, A. F. and Lekanne Deprez, R. H. (2003) Cardiomyocytes derived from embryonic stem cells resemble cardiomyocytes of the embryonic heart tube. Cardiovasc Res. 58, 399–409.
Chuva de Sousa, Lopes S.M., Hassink, R.J., Feijen, A., van Rooijen, M.A., Doevendans, P.A., Tertoolen, L., Brutel de la Riviere, A. and Mummery, C.L. (2006) Patterning the heart, a template for human cardiomyocyte development. Dev. Dyn. 235, 1994–2002.
van Laake, L. W., Hassink, R., Doevendans, P. A. and Mummery, C. (2006) Heart repair and stem cells. J. Physiol., in press.
Laflamme, M.A., Gold, J., Xu, C., Hassanipour, M., Rosler, E., Police, S., Muskheli, V. and Murry, C.E. (2005) Formation of human myocardium in the rat heart from human embryonic stem cells. Am. J. Pathol. 167, 663–671.
Xue, T., Cho, H.C., Akar, F.G., Tsang, S.Y., Jones, S.P., Marban, E., Tomaselli, G.F. and Li, R.A. (2005) Functional integration of electrically active cardiac derivatives from genetically engineered human embryonic stem cells with quiescent recipient ventricular cardiomyocytes: insights into the development of cell-based pacemakers. Circulation 111, 11–20.
Hierlihy, A.M., Seale, P., Lobe, C.G., Rudnicki, M.A. and Megeney, L.A. (2002) The post-natal heart contains a myocardial stem cell population. FEBS Lett. 530, 239–240.
Giordano, F. J., Gerber, H. P., Williams, S. P., VanBruggen, N., Bunting, S., Ruiz, Lozano, P., Gu, Y., Nath, A. K., Huang, Y., Hickey, R., et al. (2001) A cardiac myocyte vascular endothelial growth factor paracrine pathway is required to maintain cardiac function. Proc. Natl. Acad. Sci. USA 98, 5780–5785.
Gaussin, V., Van de Putte, T., Mishina, Y., Hanks, M. C., Zwijsen, A., Huylebroeck, D., Behringer, R. R. and Schneider, M. D. (2002) Endocardial cushion and myocardial defects after cardiac myocyte-specific conditional deletion of the bone morphogenetic protein receptor ALK3. Proc. Natl. Acad. Sci. USA 99, 2878–2883.
Lavine, K. J., Yu, K., White, A. C., Zhang, X., Smith, C., Partanen, J., and Ornitz, D. M. (2005) Endocardial and epicardial derived FGF signals regulate myocardial proliferation and differentiation in vivo. Dev. Cell. 8, 85–95.
Bhattacharya, S., Macdonald, S. T. and Farthing, C. R. (2006) Molecular mechanisms controlling the coupled development of myocardium and coronary vasculature. Clin. Sci. (Lond) 111, 35–46.
Yamaguchi, T. P., Dumont, D. J., Conlon, R. A., Breitman, M. L., and Rossant, J. (1993) flk-1, an flt-related receptor tyrosine kinase is an early marker for endothelial cell precursors. Development 118, 489–498.
Kataoka, H., Takakura, N., Nishikawa, S., Tsuchida, K., Kodama, H., Kunisada, T., Risau, W., Kita, T., and Nishikawa, S. I. (1997) Expressions of PDGF receptor alpha, c-Kit and Flk1 genes clustering in mouse chromosome 5 define distinct subsets of nascent mesodermal cells. Dev Growth Differ 39, 729–740.
Kouskoff, V., Lacaud, G., Schwantz, S., Fehling, H. J. and Keller, G. (2005) Sequential development of hematopoietic and cardiac mesoderm during embryonic stem cell differentiation. Proc. Natl. Acad. Sci. USA 102, 13170–13175.
Fehling, H. J., Lacaud, G., Kubo, A., Kennedy, M., Robertson, S., Keller, G. and Kouskoff, V. (2003) Tracking mesoderm induction and its specification to the hemangioblast during embryonic stem cell differentiation. Development 130, 4217–4227
Kispert, A. and Herrmann, B. G. (1993) The Brachyury gene encodes a novel DNA binding protein. Embo J 12, 3211–3220.
Kinder, S. J., Tsang, T. E., Quinlan G. A., Hadjantonakis A. K., Nagy A., and Tam P. P. (1999) The orderly allocation of mesodermal cells to the extraembryonic structures and the anteroposterior axis during gastrulation of the mouse embryo. Development 126, 4691–4701.
Nishikawa, S. I., Nishikawa, S., Hirashima, M., Matsuyoshi, N. and Kodama, H. (1998) Progressive lineage analysis by cell sorting and culture identifies FLK1+VE-cadherin+ cells at a diverging point of endothelial and hemopoietic lineages. Development 125, 1747–1757.
Yamashita, J., Itoh, H., Hirashima, M., Ogawa, M., Nishikawa, S., Yurugi, T., Naito, M., Nakao, K., and Nishikawa, S. (2000) Flk1-positive cells derived from embryonic stem cells serve as vascular progenitors. Nature 408, 92–96.
Yamashita, J. K., Takano, M., Hiraoka-Kanie, M., Shimazu, C., Peishi, Y., Yanagi, K., Nakano, A., Inoue, E., Kita, F., and Nishikawa, S. (2005) Prospective identification of cardiac progenitors by a novel single cell-based cardiomyocyte induction. FASEB J. 19,1534–1536.
Kajstura, J., Rota, M., Whang, B., Cascapera, S., Hosoda, T., Bearzi, C., Nurzynska, D., Kasahara, H., Zias, E., Bonafe, M. et al. (2005). Bone marrow cells differentiate in cardiac cell lineages after infarction independently of cell fusion. Circ. Res. 96,127–137.
Beltrami, A. P., Barlucchi, L., Torella, D., Baker, M., Limana, F., Chimenti, S., Kasahara, H., Rota, M., Musso, E., Urbanek, support myocardial regeneration. Cell 114, 763–776.
Oh, H., Bradfute, S. B., Gallardo, T. D., Nakamura, T., Gaussin, V., Mishina, Y., Pocius, J., Michael, L. H., Behringer, R. R., Garry, D. J. et al. (2003) Cardiac progenitor cells from adult myocardium: homing, differentiation, and fusion after infarction. Proc. Natl. Acad. Sci. USA 100,12313–12318.
Messina, E., DeAngelis, L., Frati, G., Morrone, S., Chimenti, S., Fiordaliso, F., Salio, M., Battaglia, M., Latronico, M. V., Coletta, M. et al. (2004) Isolation and expansion of adult cardiac stem cells from human and murine heart. Circ.Res. 95, 911–921.
Martin, C. M., Meeson, A. P., Robertson, S. M., Hawke, T. J., Richardson, J. A., Bates, S., Goetsch, S. C., Gallardo, T. D., and Garry, D. J. (2004) Persistent expression of the ATPbinding cassette transporter, Abcg2, identifies cardiac SP cells in the developing and adult heart. Dev Biol 265, 262–275.
Pfister, O., Mouquet, F., Jain, M., Summer, R., Helmes, M., Fine, A., Colucci, W. S. and Liao, R. (2005) CD31- but Not CD31+ cardiac side population cells exhibit functional cardiomyogenic differentiation. Circ. Res. 97, 52–61.
Iida, M., Heike, T., Yoshimoto, M., Baba, S., Doi, H., and Nakahata, T. (2005) Identification of cardiac stem cells with FLK1, CD31, and VE-cadherin expression during embryonic stem cell differentiation. FASEB J. 19, 371–378.
Anisimov, S. V., Tarasov, K. V., Riordon, D., Wobus, A. M. and Boheler K. R. (2002) SAGE identification of differentiation responsive genes in P19 embryonic cells induced to form cardiomyocytes in vitro. Mech. Dev. 117, 25–74.
Kaufman, D. S., Hanson, E. T., Lewis, R. L, Auerbach, R. and Thomson, J. A. (2001) Hematopoietic colony-forming cells derived from human embryonic stem cells. Proc. Natl. Acad. Sci. USA 98, 10716–10721.
Chadwick, K., Wang, L., Li, L., Menendez, P., Murdoch, B., Rouleau, A. and Bhatia, M. (2003) Cytokines and BMP-4 promote hematopoietic differentiation of human embryonic stem cells. Blood 102, 906–915.
Wang, L., Li, L., Shojaei, F., Levac, K., Cerdan, C., Menendez, P., Martin, T., Rouleau A. and Bhatia M. (2004) Endothelial and hematopoietic cell fate of human embryonic stem cells originates from primitive endothelium with hemangioblastic properties. Immunity 21, 31–41.
Ng, E. S., Davis, R. P., Azzola, L., Stanley, E.G. and Elefanty, A. G. (2005).. Forced aggregation of defined numbers of human embryonic stem cells into embryoid bodies fosters robust, reproducible hematopoietic differentiation. Blood 106, 1601–1603.
Passier, R., Ward-van Oostwaard, D., Snapper, J., Kloots, K., Hassink, R., Kuijk, E., Roelen, B., Brutel de la Riviere, A. and Mummery, C. (2005) Increased cardiomyocyte differentiation from human embryonic stem cells in serum-free cultures. Stem Cells 23, 772–780.
Menasche, P., Hagege, A. A., Vilquin, J. T., Desnos, M., Abergel, E., Pouzet, B., Bel, A., Sarateanu, S., Scorsin, M., Schwartz, K. et al. 2003. Autologous skeletal myoblast transplantation for severe postinfarction left ventricular dysfunction. J. Am. Coll. Cardiol. 41,1078–1083.
Mummery, C. L. (2005) Solace for the broken hearted. Nature 433, 585–586.
Kehat, I., Khimovich, L., Caspi, O., Gepstein, A., Shofti, R., Arbel, G., Huber, I., Satin, J., Itskovitz-Eldor, J., and Gepstein, L. (2004) Electromechanical integration of cardiomyocytes derived from human embryonic stem cells. Nat. Biotechnol. 22, 1282–1289.
Acknowledgement
A.F. is supported by the Netherlands Bsik Programme ‘stem Cells in Development and Disease’, R.P. by the EU FP6 programme ‘Heart Failure and Heart Repair’ (contract LSHM-CT-2005-018630) and A.R. by Fondation pour la Recherche Médicale. ES Cell International is thanked for the use of HES2 and HES3. We thank the Mummery group for their input.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Filipczyk, A.A., Passier, R., Rochat, A. et al. Cardiovascular development: towards biomedical applicability. Cell. Mol. Life Sci. 64, 704–718 (2007). https://doi.org/10.1007/s00018-007-6523-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00018-007-6523-2