
Abstract
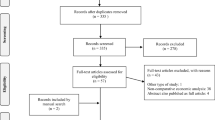
Introduction: acromegalic therapeutic goals are directed at removing the tumor, preventing tumor re-growth and reducing long-term morbidity and mortality. In this scenario, the acromegalic patient needs a variety of health resources (diagnostic tests, surgery, radiotherapy, specialist visits and drugs) for his/her cure, in order to decrease/stop the progression of the disease and to cure the co-morbid diseases. Lack of epidemiological data has suggested performing an Italian retrospective study aiming to assess the health resource consumption that is caused by acromegalic cure and the relative co-morbidities, in order to estimate the amount of the direct costs of acromegalic patients. Method: a retrospective study was performed on a total of 134 patients (142 patients selected, 76 in Genoa and 66 in Turin) for a period of about 7 yr preceding the enrolment date. Only direct costs were evaluated by performing an analysis on the perspective of Italian Healthcare Service (SSN). Results: the mean total direct costs for acromegaly cure ranged from 7.968,41 to 12.533,02 €/yr (p<0,01; Mann Whitney Test), respectively, for Responders and Non-Responders. The cost driver was drug (SS analogs) for acromegalic cure. The co-morbidity conditions associated to acromegalic Non-Responder patients are clearly higher than those with well-controlled disease. Conclusion: the study supports the hypothesis that controlled patients drove a saving for SSN in comparison to poor control patients that use more health resources.
Similar content being viewed by others

References
Melmed S. Acromegaly. N Engl J Med 1990, 322: 966–77.
Chang-DeMoranville BM, Jackson IM. Diagnosis and endocrine testing in acromegaly. Endocrinol Metab Clin North Am 1992, 21: 649–68.
Melmed S, Ezrin C, Kovacs K, et al. Acromegaly due to secretion of growth hormone by an ectopic pancreatic islet-cell tumor. N Engl J Med 1985, 312: 9–17.
Barkan AL. New options for diagnosing and treating acromegaly. Cleve Clin J Med 1998, 65: 346–9.
Thorner MO, Perryman RL, Cronin MJ, et al. Somatotroph hyperplasia. Successful treatment of acromegaly by removal of a pancreatic islet tumor secreting a growth hormone-releasing factor. J Clin Invest 1982, 70: 965–77.
Sano T, Asa SL, Kovacs K. Growth hormone-releasing hormone-producing tumors: clinical, biochemical, and morphological manifestations. Endocr Rev 1988, 9: 357–73.
Holdaway IM, Rajasoorya C. Epidemiology of acromegaly. Pituitary 1999, 2: 29–41.
Rajasoorya C, Holdaway MI, Wrightson P, et al. Determinants of clinical outcome and survival in acromegaly. Clin Endocrinol (Oxf) 1994, 41: 95–102.
Bengtsson BA, Eden S, Ernst I, et al. Epidemiology and long-term survival in acromegaly: a study of 166 cases diagnosed between 1955 and 1984. Acta Med Scand 1988, 223: 327–35.
Swearingen B, Barker FG, Katznelson L, et al. Long-term mortality after transsphenoidal surgery and adjunctive therapy for acromegaly. J Clin Endocrinol Metab 1998, 83: 3419–26.
Abosch A, Tyrrell JB, Lamborn KR, et al. Transsphenoidal microsurgery for growth hormone-secreting pituitary adenomas: Initial outcome and long-term results. J Clin Endocrinol Metab 1998, 83: 3411.
Stewart PM. Current therapy for acromegaly. Trends Endocrinol Metab 2000, 11: 128–32.
Bates AS, vant’Hoff W, Jones J, et al. An audit of outcome of treatment in acromegaly. Q J Med 1993, 86: 293–9.
Bates AS, Van’t Hott W, Jones JM, Clayton RN. Does treatment of acromegaly affect life expectancy? Metab Clin Exper 1995, 44: 1–5.
Orme SM, McNally RJQ, Cartwright RA, et al. Mortality and cancer incidence in acromegaly: a retrospective cohort study. J Clin Endocrinol Metab 1998, 83: 2730–4.
Giustina A, Barkan A, Casanueva F, et al. Criteria for cure of acromegaly: a consensus statement. J Clin Endocrinol Metab 2000, 85: 526–9.
Colao A, Merola B, Ferone D, et al. Extensive personal experience: acromegaly. J Clin Endocrinol Metab 1997, 82: 2077–81.
Stewart PM. Current therapy for acromegaly. Trends Endocrinol Metab 2000, 11: 128–32.
Ferone D, Colao A, van der Lely AJ, Lamberts SW. Pharmacotherapy or surgery as primary treatment for acromegaly? Drugs Aging 2000, 17: 81–92.
Shimon I, Melmed S. Management of pituitary tumors. Ann Intern Med 1998, 129: 472–83.
Freda PU, Wardlaw SL. Editorial: Primary medical therapy for acromegaly. J Clin Endocrinol Metab 1998, 83: 3031–3.
Yamada S, Aiba T, Takada K, et al. Retrospective analysis of long-term surgical results in acromegaly: preoperative and postoperative factors predicting outcome. Clin Endocrinol (Oxf) 1996, 82: 291–8.
Ahmed S, Elsheikh M, Page RCL, et al. Outcome of trans-sphenoidal surgery for acromegaly and its relationship to surgical experience. Clin Endocrinol (Oxf) 1999, 50: 560–7.
Clayton RN. How many surgeons to operate on acromegalic patients? Clin Endocrinol (Oxf) 1999, 50: 560–7.
Sheaves R, Jenkins P, Blackburn P, et al. Outcome of transsphenoidal surgery for acromegaly using strict criteria for surgical cure. Clin Endocrinol (Oxf) 1996, 45: 407–13.
Fahlbush R, Honegger J, Buchfelder M. Surgical management of acromegaly. Endocrinol Metab Clin North Am 1992, 21: 669–92.
Barkan AL, Halasz I, Dornfeld KJ, et al. Pituitary irradiation is ineffective in normalizing plasma insulin-like growth factor I in patients with acromegaly. J Clin Endocrinol Metab 1997, 82: 3187–91.
van der Lely AJ, de Herder WW, Lamberts SW. The role of radiotherapy in acromegaly. J Clin Endocrinol Metab 1997, 82: 3185–6.
Eastman RC, Gorden P, Roth J. Conventional supervoltage irradiation is an effective treatment for acromegaly. J Clin Endocrinol Metab 1979, 48: 931–40.
Freda PU, Wardlaw SL. Diagnosis and treatment of pituitary tumors. J Clin Endocrinol Metab 1999, 84: 3859–66.
Melmed S, Jackson I, Kleinberg D, Klibanski A current treatment guidelines for acromegaly. J Clin Endocrinol Metab 1998, 83: 2646–52.
Freda PU. Somatostatin analogs in acromegaly. J Clin Endocrinol Metab 2002, 87: 3013–8.
Cozzi R, Attanasio R, Montini M, et al. Four-Year Treatment with Octreotride-Long-Acting Repeatable in 110 Acromegalic Patients: Predictive Value of Short-Term Results? J Clin Endocrinol Metab 2003, 88: 3090–8.
van der Lely AJ, Hutson RK, Trainer PJ, et al. Long-term treatment of acromegaly with pegvisomant, a growth hormone receptor antagonist. Lancet 2001, 358: 1754–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Didoni, G., Grottoli, S., Gasco, V. et al. Cost-of-illness study in acromegalic patients in Italy. J Endocrinol Invest 27, 1034–1039 (2004). https://doi.org/10.1007/BF03345306
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03345306