
Abstract
Purpose
Recent clinical practice guidelines consider thyroid lobectomy a viable alternative for low-risk papillary thyroid carcinoma PTC measuring 1–4 cm in size. We aimed to assess the likelihood of finding postoperatively determined high-risk histopathologic features that would lead to the recommendation of completion thyroidectomy.
Methods
A retrospective review of patients who underwent total thyroidectomy for PTC measuring 1–4 cm in size between Jan 2012 and Jan 2018 was conducted. Patients with pre-operative high-risk characteristics were excluded: history of radiation exposure, positive family history, clinically suspicious cervical lymphadenopathy, and gross extrathyroidal extension (ETE). A hypothetical group of 245 patients remained eligible for lobectomy. The pathology specimens from the cancer-containing lobes were evaluated for high-risk features: aggressive histology, capsular and/or vascular invasion, microscopic ETE, and multifocality. A subgroup analysis was performed with 2 cm being the cut-off size.
Results
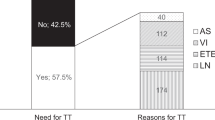
The average age was 39 years with 73% being females. Mean cancer size was 16 mm. Evaluation of the cancer-containing lobe for high-risk features revealed: aggressive histology (33%), ETE (12%), capsular invasion (33%), vascular invasion (17%), and ipsilateral multifocality (30%). The cumulative risk of having ≥1 high-risk feature mandating completion thyroidectomy was 59%. The risk was considerably higher for lesions ≤2 cm compared to larger lesions (64% vs.48%; p = 0.049; RR = 1.3).
Conclusions
A considerable proportion of patients initially eligible for lobectomy have high-risk features that only become evident at pathology. Therefore, a comprehensive approach is advocated to determine the extent of surgery for PTC incorporating patient preferences regarding risks and benefits.
Similar content being viewed by others


Data availability
The data supporting the findings of this study are available from the corresponding author upon request.
References
C. La Vecchia, M. Malvezzi, C. Bosetti, W. Garavello, P. Bertuccio, F. Levi, E. Negri, Thyroid cancer mortality and incidence: a global overview. Int. J. Cancer 136, 2187–2195 (2015). https://doi.org/10.1002/ijc.29251
C. Spinelli, S. Strambi, S. Bakkar, A. Nosiglia, G. Elia, A. Bertocchini, C. Calani, M. Leoni, R. Morganti, G. Materazzi, Surgical management of diffuse sclerosing variant of papillary thyroid carcinoma. Experience in 25 patients. World J. Surg. 44, 155–162 (2020). https://doi.org/10.1007/s00268-019-05230-5
F. Nabhan, M.D. Ringel, Thyroid nodules and cancer management guidelines: comparisons and controversies. Endocr. Relat. Cancer 24, R13–R26 (2017). https://doi.org/10.1530/ERC-16-0432
B.R. Haugen, E.K. Alexander, K.C. Bible et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid 26, 1–133 (2016). https://doi.org/10.1089/thy.2015.0020.7
R.M. Tuttle, B. Haugen, N.D. Perrier, Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition): What Changed and Why? Thyroid 27, 751–756 (2017). https://doi.org/10.1089/thy.2017.0102
P. Miccoli, S. Bakkar, Surgical management of papillary thyroid carcinoma: an overview. Updates Surg. 69, 145–150 (2017). https://doi.org/10.1007/s13304-017-0449-5
S. Bakkar, T.S. Papavramidis, Q. Aljarrah, G. Materazzi, P. Miccoli, Energy-based devices in thyroid surgery—an overview. Gland. Surg. 9(Suppl 1), S14–S17 (2020). https://doi.org/10.21037/gs.2019.08.05
S. Bakkar, E. Macerola, Q. Aljarrah, A. Proietti, G. Materazzi, F. Basolo, P. Miccoli, BRAFV600E mutation: a potential predictor of more than a Sistrunk’s procedure in patients with thyroglossal duct cyst carcinoma and a normal thyroid gland. Updates Surg. 71, 701–704 (2019). https://doi.org/10.1007/s13304-019-00684-7
S. Bakkar, K. Al-Omar, Q. AL-Jarrah, M. Al-Dabbas, N. Al-Dabbas, S. Samara, P. Miccoli, Impact of COVID-19 on thyroid cancer surgery and adjunct therapy. Updates Surg. 72, 867–869 (2020). https://doi.org/10.1007/s13304-020-00833-3
K.Y. Bilimoria, D.J. Bentrem, C.Y. Ko, A.K. Stewart, D.P. Winchester, M.S. Talamonti, C. Sturgeon, Extent of surgery affects survival for papillary thyroid cancer. Ann. Surg. 246, 375–381 (2007)
American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, D.S. Cooper, G.M. Doherty, B.R. Haugen, R.T. Kloos, S.L. Lee, S.J. Mandel, E.L. Mazzaferri, B. McIver, F. Pacini, M. Schlumberger, S.I. Sherman, D.L. Steward, R.M. Tuttle, Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 19, 1167–1214 11 (2009)
M.A. Adam, J. Pura, L. Gu, M.A. Dinan, D.S. Tyler, S.D. Reed, R. Scheri, S.A. Roman, J.A. Sosa, Extent of surgery for papillary thyroid cancer is not associated with survival: an analysis of 61,775 patients. Ann. Surg. 260, 601–615 (2014)
M.A. Adam, J. Pura, P. Goffredo, M.A. Dinan, T. Hyslop, S.D. Reed, R.P. Scheri, S.A. Roman, J.A. Sosa, Impact of extent of surgery on survival for papillary thyroid cancer patients younger than 45 years. J. Clin. Endocrinol. Metab. 100, 115–121 (2015). https://doi.org/10.1210/jc.2014-3039
Edge S., Byrd D. R., Compton C. C., Fritz A. G., Greene F. L., Trotti A. (eds) AJCC Cancer Staging Manual, 7th edn. Springer, New York (2010).
J.B. Choi, S.G. Lee, M.J. Kim, T.H. Kim, E.J. Ban, C.R. Lee, J. Lee, S.W. Kang, J.J. Jeong, K.H. Nam, W.Y. Chung, C.S. Park, Oncologic outcomes in patients with 1-cm to 4-cm differentiated thyroid carcinoma according to extent of thyroidectomy. Head. Neck 41, 56–63 (2019). https://doi.org/10.1002/hed.25356
R. Sawant, K. Hulse, S. Sohrabi, J.C.L. Yeo, K. Pal, F.W. Gibb, R. Adamson, I.J. Nixon, The impact of completion thyroidectomy. Eur. J. Surg. Oncol. 45, 1171–1174 (2019). https://doi.org/10.1016/j.ejso.2019.03.018
Author contributions
Corresponding author S.B.: study concept and design, data interpretation, article writing, final approval, accountability for all aspects of the work. K.A., G.D., Q.A. and T.P.: data collection and interpretation, final approval, accountability for all aspects of the work. G.M., P.M.: critical revision, final approval, accountability for all aspects of the work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For this type of study formal consent is not required.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bakkar, S., Al-Omar, K., Donatini, G. et al. Postoperatively determined high-risk histopathologic features in papillary thyroid carcinoma initially eligible for thyroid lobectomy: a game changer. Endocrine 74, 611–615 (2021). https://doi.org/10.1007/s12020-021-02788-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-021-02788-w