
Aim:
The standard treatment for patients with clinically resectable rectal cancer is surgery. Postoperative radiochemotherapy is recommended for patients with advanced disease (pT3/4 or pN+). In recent years, encouraging results of preoperative radiotherapy have been reported. This prospective randomized phase-III trial (CAO/ARO/AIO-94) compares the efficacy of neoadjuvant radiochemotherapy to standard postoperative radiochemotherapy. We report on the design of the study and first results with regard to toxicity of radiochemotherapy and postoperative morbidity.
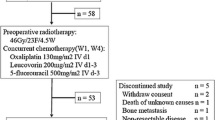
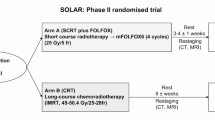
Patients and Methods: Patients with locally advanced operable rectal cancer (uT3/4 or uN+, Mason CS III/IV) were randomly assigned to pre- or postoperative radiochemotherapy: A total dose of 50.4 Gy (single dose 1.8 Gy) was applied to the tumor and the pelvic lymph nodes. 5-FU (1,000 mg/m2/d) was administered concomitantly in the first and fifth week of radiation as 120-h continuous infusion. Four additional cycles of 5-FU chemotherapy (500 mg/m2/d, iv bolus) were applied. Radiochemotherapy was identical in both arms except for a small-volume boost of 5.4 Gy in the postoperative setting. Time interval between radiochemotherapy and surgery was 4–6 weeks in both arms. Techniques of surgery were standardized and included total mesorectal excision. In addition, stratification according to surgeons involved has been provided for. Primary endpoints of the study are 5-year overall-survival, local and distant control, secondary endpoints include rate of curative (R0) resections and sphincter saving procedures, toxicity of radiochemotherapy, surgical complications and quality of life.
Results: As of 15th November 2000, 628 patients were randomized from 26 participating institutions: 310 patients were randomized to postoperative radiochemotherapy, 318 patients to preoperative radiochemotherapy. Acute toxicity (WHO) of radiochemotherapy was low, with less than 15% of patients experiencing Grade 3 or higher toxicity: The principal toxicity was diarrhea, with 12% in the postoperative radiochemotherapy arm and 10% in the preoperative radiochemotherapy arm having Grade-3, and 1% in either arm having Grade 4 diarrhea. Erythema, nausea and leukopenia were the next common toxicities, with less than 3% of patients in either arm suffering Grade 3 or greater leukopenia or nausea. Postoperative complication rates were similar in both arms, with 12% (postoperative radiochemotherapy) and 13% (preoperative radiochemotherapy) of patients, respectively, suffering from anastomotic teakage, 4% (postoperative radiochemotherapy) and 3% (preoperative radiochemotherapy) from postoperative bleeding, and 6% (postoperative radiochemotherapy) and 5% (preoperative radiochemotherapy) from delayed wound healing.
Conclusion: The patient accrual of our trial is satisfactory, neoadjuvant radiochemotherapy is well tolerated and bears no higher risk for postoperative morbidity.
Ziel:
Die Standardbehandlung des operablen Rektumkarzinoms ist die sofortige Operation. Eine postoperative Radiochemotherapie wird für Patienten mit fortgeschrittenen Tumoren (pT3/4 oder pN+) empfohlen. In den letzten Jahren wurden vielversprechende Ergebnisse durch eine präoperative Bestrahlung erzielt. Wir beschreiben das Design einer prospektiv randomisierten Phase-III-Studie (CAO/ARO/AIO-94), die die Wirksamkeit einer neoadjuvanten Radiochemotherapie mit der postoperativen Standardbehandlung vergleicht, und berichten über erste Ergebnisse zur Toxizität der Radiochemotherapie und zur postoperativen Komplikationsrate.
Patienten und Methoden: Patienten mit lokal fortgeschrittenem operablen Rektumkarzinom (uT3/4 oder uN+, Mason CS III/IV) wurden auf den prä- oder postoperativen Radiochemotherapiearm randomisiert: Tumor(-bett) und pelvines Lymphabflussgebiet erhielten 50,4 Gy (Einzeldosis: 1,8 Gy). In der ersten und fünften Bestrahlungswoche erfolgte eine simultane 5-FU-Chemotherapie in einer Dosierung von 1000 mg/m2/Tag, appliziert als 120-stündige Dauerinfusion. Vier weitere Zyklen 5-FU (500 mg/m2/Tag, appliziert als Bolusgabe) schlossen sich an. Das Radiochemotherapieregime war in beiden Armen (bis auf einen Boost von 5,4 Gy im postoperativen Radiochemotherapiearm) identisch. Das Intervall zwischen Radiochemotherapie und Operation betrug in beiden Armen 4–6 Wochen. Die Operationstechnik war standardisiert und beinhaltete die totale Entfernung des Mesorektums. Außerdem erfolgte eine Stratifizierung nach beteiligten Chirurgen. Primäre Endpunkte der Studie sind das 5-Jahres-Überleben, die lokale und systemische Tumorkontrolle; sekundäre Endpunkte umfassen die Rate an R0-Operationen und kontinenzerhaltenden Verfahren, die Toxizität der Radiochemotherapie, die postoperative Komplikationsrate und die Lebensqualität.
Ergebnisse: Bis 15. November 2000 wurden 628 Patienten in 26 beteiligten Zentren randomisiert: 310 Patienten in den postoperativen Radiochemotherapiearm, 318 Patienten in den präoperativen Radiochemotherapiearm. Die Akuttoxizität war insgesamt gering; bei weniger als 15% der Patienten trat eine Grad-3 oder -4-Toxizität nach WHO auf. Die häufigste Nebenwirkung war die Diarrhö, die mit Grad 3 bzw. 4 bei 12% bzw. 1% im postoperativen Arm und mit 10% bzw. 1% im präoperativen Arm auftrat. Hauterythem, Übelkeit und Leukopenie waren weitere häufige Nebenwirkungen, Grad-3-Leukopenie und Übelkeit wurden bei weniger als 3% beobachtet. Die postoperative Komplikationsrate war in beiden Armen ähnlich; nach sofortiger Operation (postoperative Radiochemotherapie) entwickelten 12% der Patienten, nach präoperativer Radiochemotherapie 13% eine Anastomoseninsuffizienz, bei 4% (postoperative Radiochemotherapie) und 5% (präoperative Radiochemotherapie) Wundheilungsstörungen auf.
Schlussfolgerung: Die Patientenrekrutierung verläuft sehr zufriedenstellend. Die neoadjuvante Radiochemotherapie wird gut toleriert und erhöht die postoperative Komplikationsrate nicht.
Similar content being viewed by others

Author information
Authors and Affiliations
Additional information
Received: January 2, 2001; accepted: January 24, 2001
Rights and permissions
About this article
Cite this article
Sauer, R., Fietkau, R., Wittekind, C. et al. Adjuvant versus Neoadjuvant Radiochemotherapy for Locally Advanced Rectal Cancer A Progress Report of a Phase-III Randomized Trial (Protocol CAO/ARO/AIO-94). Strahlenther Onkol 177, 173–181 (2001). https://doi.org/10.1007/PL00002396
Issue Date:
DOI: https://doi.org/10.1007/PL00002396