
Abstract
Background
A context-specific, spatial-temporal understanding of a chain of tuberculosis (TB) transmission can inform TB elimination strategy.
Methods
Clinical, public health and molecular epidemiologic data were used to: 1) identify and describe a complex cluster of TB cases in Alberta, 2) elucidate transmission sequences, and 3) assess case-patient mobility. Socio-economic indicators in loci of transmission and the province at large were described. Factors seen to be fostering or hampering TB elimination were identified.
Results
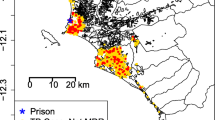
Over a 15-year period, 18 TB cases in Alberta and multiple cases in the Northwest Territories were determined to be due to the same strain. One patient was diagnosed at death; all others completed directly-observed therapy (DOT). Case-level analysis revealed that patients were highly mobile with transmission of the strain over 26,569 km2, an average of 2.8 different places of residence per patient during treatment, and contacts of sputum smear-positive cases spanning 9 of 17 regional health authorities. The majority of the contacts (57%) were attached to a single infectious case living in a homeless shelter. The three loci of transmission in Alberta were separated geographically but similar in terms of median incomes, rates of unemployment, levels of post-secondary education, and rates of population mobility (p<0.0001).
Conclusion
Upon review of the experience, central oversight, intra- and inter-jurisdictional coordination and DOT were seen as fostering, and the absence of ‘real-time’ DNA fingerprinting, social network analysis, engineering controls in shelters and better determinants of health in loci of transmission were seen as hampering TB elimination.
Résumé
Contexte
La connaissance spatio-temporelle et contextuelle d’une chaîne de transmission de la tuberculose pourrait étayer la stratégie d’élimination de cette maladie.
Méthode
À l’aide de données cliniques, de santé publique et d’épidémiologie moléculaire, nous avons: 1) mis en évidence et décrit une concentration complexe de cas de tuberculose en Alberta, 2) élucidé les séquences de transmission et 3) évalué la mobilité des cas patients. Nous décrivons les indicateurs socioéconomiques sur les lieux de transmission et dans le reste de la province. Les facteurs qui semblent favoriser ou entraver l’élimination de la tuberculose sont indiqués.
Résultats
Sur une période de 15 ans, il a été déterminé que 18 cas de tuberculose relevés en Alberta et plusieurs cas dans les Territoires du Nord-Ouest avaient la même souche. L’un des patients a été diagnostiqué après sa mort; tous les autres ont reçu un traitement directement observé (TDO). L’analyse par cas montre que les patients étaient très mobiles: la souche s’est propagée sur 26 569 km2, chaque patient a eu en moyenne 2,8 lieux de résidence durant son traitement, et les contacts des cas dont les frottis de crachat étaient positifs couvraient 9 des 17 régies régionales de la santé. La majorité des contacts (57 %) étaient rattachés à un même cas infectieux hébergé dans une maison pour sans-abri. Les trois lieux de transmission en Alberta étaient éloignés géographiquement, mais semblables pour ce qui est des revenus médians, des taux de chômage, des niveaux d’études postsecondaires et des taux de mobilité de la population (p<0,0001).
Conclusion
Selon notre analyse, les facteurs favorisant l’élimination de la tuberculose sont la surveillance centrale, la coordination intra- et interprovinciale et le TDO. Les facteurs entravant l’élimination de la tuberculose sont l’absence d’identification „ en temps réel ” par le code génétique, l’absence d’analyse des réseaux sociaux, l’absence de mesures techniques dans les maisons de refuge et l’absence de meilleurs déterminants de la santé dans les lieux de transmission.
Similar content being viewed by others

References
Stop TB Partnership and World Health Organization. Global Plan to Stop TB 2006–2015. WHO/HTM?STB/2006.35. Geneva, Switzerland: World Health Organization, 2006.
The Canadian Lung Association and the Public Health Agency of Canada. The Canadian Tuberculosis Standards, 6th Edition, 2007. Available at: https://doi.org/www.publichealth.gc.ca/tuberculosis (Accessed August 4, 2009).
Barnes P, Cave D. Molecular epidemiology of tuberculosis. N Engl J Med 2003;349:1149–56.
Nolan CM, Elarth AM, Barr H, Saeed AM, Risser DR. An outbreak of tuberculosis in a shelter for homeless men. A description of its evolution and control. Am Rev Respir Dis 1991;143:257–61.
Barnes P, El-Hajj H, Preston-Martin S, Cave D, Jones BE, Otaya M, et al. Transmission of tuberculosis among the urban homeless. JAMA 1996;275:305–7.
Curtis AB, Ridzon R, Novick LF, Driscoll J, Blair D, Oxtoby M, et al. Analysis of Mycobacterium tuberculosis transmission patterns in a homeless shelter outbreak. Int J Tuberc Lung Dis 2000;4:308–13.
Lathan M, Mukasa LN, Hooper N, Golub J, Baruch N, Mulcahy D, et al. Cross-jurisdictional transmission of Mycobacterium tuberculosis in Maryland and Washington, DC, 1996–2000, linked to the homeless. Emerg Inf Dis 2002;8:1249–51.
Klovdahl AS, Graviss EA, Yaganehdoost A, Ross MW, Wanger A, Adams GJ, et al. Networks and tuberculosis: An undetected community outbreak involving public places. Soc Sci Med 2001;52:681–94.
van Embden JDA, Cave MD, Crawford JT, Dale JW, Eisenach KD, Gicquel B, et al. Strain identification of Mycobacterium tuberculosis by DNA fingerprinting: Recommendations for standardized methodology. J Clin Microbiol 1993;31:406–9.
van Soolingen D. Molecular epidemiology of tuberculosis and other mycobac-terial infections: Main methodologies and achievements. J Intern Med 2001;249:1–26.
FitzGerald JM, Fanning A, Hoeppner V, Hershfield E, Kunimoto D and the Canadian Molecular Epidemiology of TB Study Group. The molecular epidemiology of tuberculosis in Western Canada. Int J Tuberc Lung Dis 2003;7:132–38.
Long R, Whittaker D, Russell K, Kunimoto D, Reid R, Fanning A, et al. Pedi-atric tuberculosis in Alberta First Nations (1991-2000): Outbreaks and the protective effect of Bacille Calmette-Guérin (BCG) vaccine. Can J Public Health 2004;95:249–55.
Public Health Agency of Canada. Tuberculosis in Canada 2007 — Pre-release. Available at: https://doi.org/www.publichealth.gc.ca/tuberculosis (Accessed August 4, 2009).
Centers for Disease Control and Prevention. Guidelines for the investigation of contacts of persons with infectious tuberculosis. MMWR 2005;54(RR15):1–37.
Long R. Tuberculosis control in Alberta. Can J Public Health 2002;93:264–66.
Mah MW, Fanning EA. An epidemic of primary tuberculosis in a Canadian Aboriginal community. Can J Infect Dis 1991;2:133–41.
Marks SM, Taylor Z, Qualls NL, Shrestha-kuwahara RJ, Wilce MA, Nguyen CH. Outcomes of contact investigations of infectious tuberculosis patients. Am J Respir Crit Care Med 2000;162:2033–38.
Šebek M. DNA finger printing and contact investigation. Int J Tuberc Lung Dis 2000;4(2):S45–S48.
Reichler MR, Reves R, Bur S, Thompson V, Mangura BT, Ford J, et al. Evaluation of investigations conducted to detect and prevent transmission of tuberculosis. JAMA 2002;287:991–95.
Mohle-Boetani JC, Flood J. Contact investigations and the continued commitment to control of tuberculosis. JAMA 2002;287:1040–42.
Weis S. Contact investigations. How do they need to be designed for the 21st century? Am J Respir Crit Care Med 2002;166:1016–17.
Daley CL, Kawamura LM. The role of molecular epidemiology in contact investigations: A US perspective. Int J Tuberc Lung Dis 2003;7:S458–S462.
Dunlap NE. The use of RFLP as a tool for tuberculosis control: Utility or futility. Int J Tuberc Lung Dis 2000;4(12):S134–S138.
Sterling TR, Thompson D, Stanley RL, McElroy PD, Madison A, Moore K, et al. A multi-state outbreak of tuberculosis among members of a highly mobile social network: Implications for tuberculosis elimination. Int J Tuberc Lung Dis 2000;4:1066–73.
McElroy PD, Rothenberg RB, Varghese R, Woodruff R, Minns GO, Muth SQ, et al. A network-informed approach to investigating a tuberculosis outbreak: Implications for enhancing contact investigations. Int J Tuberc Lung Dis 2003;7(Suppl 3):S486–S493.
van Deutekom H, Hoijng SP, de Haas PEW, Langendam MW, Horsman A, van Soolingen D, et al. Clustered tuberculosis cases — Do they represent recent transmission and can they be detected earlier? Am J Respir Crit Care Med 2004;169:806–10.
Fitzpatrick LK, Hardacker JA, Heirendt W, Agerton T, Streicher A, Melnyk H, et al. A preventable outbreak of tuberculosis investigated through an intricate social network. Clin Infect Dis 2001;33:1801–6.
Cook VJ, Sun SJ, Tapia J, Muth SQ, Argüello F, Lewis BL, et al. Transmission network analysis in tuberculosis contact investigations. JID 2007;196:1517–27.
Norris MJ, Cooke N, Clatworthy S. Aboriginal mobility and migration patterns and the policy implications. In: White JP, Maxim PS, Beavon D (Eds.), Aboriginal Conditions: Research as a Foundation for Public Policy. Vancouver, BC: UBC Press, 2003;108–29.
Escombe AR, Moore DAJ, Gilman RH, Navincopa M, Ticona E, Mitchell B, et al. Upper room ultraviolet light and negative air ionization to prevent tuberculosis transmission. PLoS Med 2009;6:e1000043. doi:10.1371/journal.pmed.1000043.
Rendleman NJ. Mandated tuberculosis screening in a community of homeless people. Am J Prev Med 1999;17:108–13.
Kimmerling ME, Shakes CF, Carlisle R, Lok KH, Benjamin WH, Dunlap NE. Spot sputum screening: Evaluation of an intervention in two homeless shelters. Int J Tuberc Lung Dis 1999;3:613–19.
Moro ML, Salamina G, Gori A, Penati V, Sacchetti R, Mezzetti F, et al. Two-year population-based molecular epidemiological study of tuberculosis transmission in the metropolitan area of Milan, Italy. Eur J Clin Microbiol 2002;21:114–22.
Oeltmann JE, Kammerer JS, Pevzner ES, Moonan PK. Tuberculosis and substance abuse in the United States, 1997–2006. Arch Int Med 2009;169:189–97.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by grants from the Aboriginal Health Strategy Project Fund, Alberta Health and Wellness, and First Nations and Inuit Health, Health Canada, Alberta Region.
This work was prepared in partial fulfillment of a Master’s of Science degree in Public Health by Anne Aspler.
Conflict of Interest: None to declare.
Rights and permissions
About this article
Cite this article
Aspler, A., Chong, H., Kunimoto, D. et al. Sustained Intra- and Inter-jurisdictional Transmission of Tuberculosis within a Mobile, Multi-ethnic Social Network: Lessons for Tuberculosis Elimination. Can J Public Health 101, 205–209 (2010). https://doi.org/10.1007/BF03404391
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03404391