
Abstract
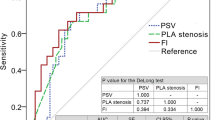
General dynamic penile color doppler ultrasound (D-PCDU) screening in patients with erectile dysfunction (ED) has been questioned due to an inadequate cost-benefit ratio. The aim of the present study is to evaluate the validity of different risk scores in the identification of patients being screened for arteriogenic ED (AED) at D-PCDU. A consecutive series of 738 patients with ED was studied. AED was defined when peak systolic velocity (PSV) was lower than 25 cm/sec. The assessment of cardiovascular risk was evaluated using different risk engines, derived from the Framingham, the PROCAM and the Progetto Cuore studies. An iterative receiver operator characteristic (ROC) curve analysis was used to determine the most proper threshold for different scales for the screening of AED. Among the patients studied, 52 (7%) had PSV<25 cm/sec. The area under the ROC curves for pathological PSV in relation to cardiovascular risk estimated with different engines was 0.762±0.03, 0.716±0.03, and 0.667±0.03 for Progetto Cuore, Framingham, and PROCAM engines, respectively. Sensitivity and specificity of Progetto Cuore estimated risk were 67%, 71 % when a threshold of 15% was chosen. Corresponding figures for Framingham and PROCAM engine were 74%, 57% and 69%, 55%, respectively. If D-PCDU is performed only on patients with cardiovascular risk >15%, who represent about 1/4 of all patients (26.8%), as estimated by Progetto Cuore, about 70% of cases of arteriogenic ED can be identified. Estimated cardiovascular risk, assessed through risk engines, could be used to identify patients who should undergo D-PCDU evaluation for the diagnosis of AED.
Similar content being viewed by others

References
NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA 1993, 270: 83–90.
Corona G, Petrone L, Mannucci E, et al. Assessment of the relational factor in male patients consulting for sexual dysfunction: the concept of couple sexual dysfunction. J Androl 2006, 27: 795–801.
Corona G, Mannucci E, Schulman C, et al. Psychobiologic correlates of the metabolic syndrome and associated sexual dysfunction. Eur Urol 2006, 50: 595–604.
Corona G, Mannucci E, Petrone L, et al. Psycho-biological correlates of free-floating anxiety symptoms in male patients with sexual dysfunctions. J Androl 2006, 27: 86–93.
Petrone L, Mannucci E, Corona G, et al. Structured interview on erectile dysfunction (SIEDY): a new, multidimensional instrument for quantification of pathogenetic issues on erectile dysfunction. Int J Impot Res 2003, 15: 210–20.
Wespes E, Amar E, Hatzichristou D, et al; EAU. EAU Guidelines on erectile dysfunction: an update. Eur Urol 2006, 49: 806–15.
Burnett AL. Erectile dysfunction. J Urol 2006, 175 (3 Pt 2): S25–31.
Montorsi P, Ravagnani PM, Galli S, et al. Association between erectile dysfunction and coronary artery disease: Matching the right target with the right test in the right patient. Eur Urol 2006, 50: 721–31.
Montorsi F, Briganti A, Salonia A, et al. Erectile dysfunction prevalence, time of onset and association with risk factors in 300 consecutive patients with acute chest pain and angiographically documented coronary artery disease. Eur Urol 2003, 44: 360–4.
Montorsi P, Ravagnani PM, Galli S, et al. The artery size hypothesis: a macrovascular link between erectile dysfunction and coronary artery disease. Am J Cardiol 2005, 96: 19M–23M.
Thompson IM, Tangen CM, Goodman PJ, Probstfield JL, Moinpour CM, Coltman CA. Erectile dysfunction and subsequent cardiovascular disease. JAMA 2005 21, 294: 2996–3002.
Wilkins CJ, Sriprasad S, Sidhu PS. Colour Doppler ultrasound of the penis. Clin Radiol 2003, 58: 514–23.
Golijanin D, Singer E, Davis R, Bhatt S, Seftel A, Dogra V. Doppler evaluation of erectile dysfunction — part 1. Int J Impot Res 2007, 19: 37–42.
Golijanin D, Singer E, Davis R, Bhatt S, Seftel A, Dogra V. Doppler evaluation of erectile dysfunction — part 2. Int J Impot Res 2007, 19: 43–8.
Aversa A, Sarteschi LM. The role of penile colour-duplex ultrasound for the evaluation of erectile dysfunction. J Sex Med 2007, 4: 1437–47.
Broderick GA, Lue TF. Evaluation and nonsurgical management of erectile dysfunction and priapism. In: Walsh PC, Retik AB, Darracott Vaughan E, Wein AJ eds. Campbell’s Urology 8th ed. Elsevier Science: Philadelphia (USA). 2002, 1589–671.
Lewis RW, King BF. Dynamic color Doppler sonography in the evaluation of penile erectile disorders. Int J Impot Res 1994, 6: A30 (abstract).
Rhee E, Osborn A, Witt M. The correlation of cavernous systolic occlusion pressure with peak velocity flow using color duplex Doppler ultrasound. J Urol 1995, 153: 358–60.
Seftel AD. Diagnosis of Erectile Dysfunction. In: Porst H, Buvat J eds. Standard Practice in Sexual Medicine. Malden (USA): Blackwell Publishing. 2006, 59–73.
Allen RP, Engel RM, Smolev JK, Brendler CB. Comparison of duplex ultrasonography and nocturnal penile tumescence in evaluation of impotence. J Urol 1994, 151: 1525–9.
Slob AK, Cornelissen S, Dohle GR, Gijs L, van der Werff ten Bosch JJ. The limited practical value of color Doppler sonography in the differential diagnosis of men with erectile dysfunction. Int J Impot Res 2002, 14: 201–3.
Shamloul R. Peak systolic velocities may be falsely low in young patients with erectile dysfunction. J Sex Med 2006, 3: 138–43.
Mancini M, Bartolini M, Maggi M, Innocenti P, Forti G. The presence of arterial anatomical variations can affect the results of duplex sonographic evaluation of penile vessels in impotent patients. J Urol 1996, 155: 1919–23.
Crown S, Crisp AH. Ashort clinical diagnostic self-rating scale for psychoneurotic patients. The Middlesex Hospital Questionnaire (M.H.Q.). Br J Psychiatry. 1966, 112: 917–23.
Anderson KM, Wilson PW, Odell PM, Kannel WB. An updated coronary risk profile. A statement for health professionals. Circulation 1991, 83: 356–62.
Assmann G, Cullen P, Schulte H. Simple scoring scheme for calculating the risk of acute coronary events based of the 10-year followup of the prospective cardiovascular Munster (PROCAM) study. Circulation 2002, 105: 310–5.
Palmieri L, Panico S, Vanuzzo D, et al; Gruppo di Ricerca del Progetto CUORE. Evaluation of the global cardiovascular absolute risk: the Progetto CUORE individual score. Ann Ist Super Sanita 2004, 40: 393–9.
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285: 2486–97.
Corona G, Mannucci E, Petrone L, et al. NCEP-ATPIII-defined metabolic syndrome, type 2 diabetes mellitus, and prevalence of hypogonadism in male patients with sexual dysfunction. J Sex Med 2007, 4: 1038–45.
Corona G, Mannucci E, Petrone L, et al. A comparison of NCEP-AT-PIII and IDF metabolic syndrome definitions with relation to metabolic syndrome-associated sexual dysfunction. J Sex Med 2007, 4: 789–96.
McVary KT. Clinical practice. Erectile dysfunction. N Engl J Med 2007, 357: 2472–81.
Montague DK, Jarow JP, Broderick GA, et al. Chapter 1: The management of erectile dysfunction: an AUA update. J Urol 2005, 174: 230–9.
Hackett G, Kell P, Ralph D, et al; British Society for Sexual Medicine. British Society for Sexual Medicine Guidelines on the Management of Erectile Dysfunction. J Sex Med 2008, 5: 1841–65.
Foresta C, Caretta N, Aversa A, et al. Erectile dysfunction: symptom or disease? J Endocrinol Invest 2004, 27: 80–95.
Kostis JB, Jackson G, Rosen R, et al. Sexual dysfunction and cardiac risk (the Second Princeton Consensus Conference). Am J Cardiol 2005, 96: 85M–93M.
Conroy RM, Pyörälä K, Fitzgerald AP, et al; SCORE project group. Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J 2003, 24: 987–1003.
Whitfield MD, Gillett M, Holmes M, Ogden E. Predicting the impact of population level risk reduction in cardio-vascular disease and stroke on acute hospital admission rates over a 5 year period — pilot study. Public Health 2006, 120: 1140–8.
D’Agostino RB Sr, Grundy S, Sullivan LM, Wilson P; CHD Risk Prediction Group. Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation. JAMA 2001, 286: 180–7.
Pyörälä K.Assessment of coronary heart disease risk in populations with different levels of risk. Eur Heart J 2000, 21: 348–50.
Hense HW, Schulte H, Lowel H, Assmann G, Keil U. Framingham risk function overestimates risk of coronary heart disease in men and women from Germany—results from the MONICA Augsburg and the PROCAM cohorts. Eur Heart J 2003, 24: 937–45.
Menotti A, Puddu PE, Lanti M. Comparison of the Framingham risk function-based coronary chart with risk function from an Italian population study. Eur Heart J 2000, 21: 365–70.
Author information
Authors and Affiliations
Corresponding author
Additional information
G. Corona and E. Mannucci contributed equally to the paper.
Rights and permissions
About this article
Cite this article
Corona, G., Mannucci, E., Fisher, A.D. et al. Cardiovascular risk engines can help in selecting patients to be evaluated by dynamic penile color doppler ultrasound. J Endocrinol Invest 31, 1058–1062 (2008). https://doi.org/10.1007/BF03345652
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03345652