
Summary
The German nosocomial infections surveillance system KISS was established in 1996 using a surveillance protocol based on the National Nosocomial Infections Surveillance (NNIS) System. Meanwhile data from a total of 274 intensive care units (ICU) are available, among them 134 interdisciplinary, 71, surgical, 55 medical, 9 neurosurgical and 5 paediatric ICUs. The data comprise about 6,966 surveillance months with more than 500,000 intensive care patients and more than 1.8 million patient days. A total of 6,888 cases of pneumonia and 2,357 cases of central venous catheter (CVC) associated primary bloodstream infections (BSI) were recorded.
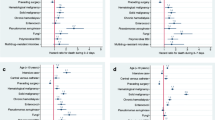
Ventilator associated pneumonia rates and CVC associated primary BSI rates are presented, stratified according to the type of the ICU and affiliation to a university, a teaching hospital or another type of hospital.
The most frequent pathogens associated with ventilator associated pneumonia wereS. aureus (24.1%), followed byP. aeruginosa (16.8%) and Klebsiella spp. (12.1%). In the case of CVC associated primary BSI coagulase negative staphylococci dominated (30.9%) followed byS. aureus (15.4%) and Enterococci spp. (11.6%). A remarkable increase of Methicillin Resistant Staphylococcus aureus (MRSA) infections was observed during the period from 1997 to 2002, 19.2% ofS. aureus associated pneumonia cases and 25.5% ofS. aureus associated primary BSI were due to MRSA.
KISS data are useful benchmarks for internal quality management, however a careful interpretation is necessary to stimulate infection control efforts.
Zusammenfassung
Das Krankenhaus-Infektions-Surveillance-System KISS wurde im Jahr 1996 auf der Basis der Methoden des amerikanischen National Nosocomial Infections Surveillance (NNIS) Systemes etabliert. Mittlerweile beinhaltet es Daten von 274 Intensivstationen darunter 134 interdisziplinäre 71 chirurgische, 55 medizinische, 9 neurochirurgische und 5 pädiatrische Intensivstationen. Wir haben einen Überblick über 6966 Beobachtungsmonate mit mehr als 500.000 Intensivpatienten und mehr als 1,8 Millionen Patiententagen. Es wurden 6888 beatmungsassozilierte Pneumonien und 2357 Zentralvenenkatheter (ZVK)-assoziierte Sepsis-Fälle erfasst.
Die beatmungsassoziierten Pneumonieraten und ZVK-assoziierten primären Sepsisraten werden nach Art der Intensivstation und Status des zugehörigen Krankenhauses stratifiziert präsentiert.
Bei beatmungsassoziierten Pneumonien sindS. aureus die häufigsten Erreger mit einem Anteil von 24,1% aller Fälle, gefolgt vonP. aeruginosa (16,8%) und Klebsiella spp. (12,1%). Im Fall der ZVK-assoziierten Sepsis werden vor allem koagulasenegative Staphylokokken gefunden (30.9%) gefolgt vonS. aureus (15,4%) und Enterococcus spp. (11,6%). Ein bemerkenswerter Anstieg der Methicillin-resistenten Staphylococcus aureus (MRSA) wurde im Zeitraum 1997 bis 2002 beobachtet. Bei denS. aureus-beciigten beatmungsassoziierten Pneumonien beträgt der Anteil der MRSA 19,2%. Bei denS. aureus bedingten Sepsisfällen liegt der MRSA-Anteil bei 25,5%
Die KISS-Daten liefern wertvolle Benchmark-Information für das interne Qualitätsmanagement, allerdings ist eine sorgfälitge Interpretation notwendig, um Präventionsmaßnahmen zu stimulieren.
Article PDF
Similar content being viewed by others

Literatur
American Society of Healthcare Pharmacists (1999)
Anonym (2002) Guidelines for the prevention of intravascular catheter-related infections. Morbidity and Mortality Weekly Report 51: RR-10
CDC (2002) Draft Guideline for prevention of healthcare associated pneumonia, 2002. www.ede. gov (2002)
Emori TG, Culver DH, Horan TC, jarvis W, White J, Olson D, et al. (1991) National Nosocomial Infection Surveillance System (NNIS): description of surveillance methodology. Am J Infect Control 19: 19–35
NRZ. http://www.nrz-hygiene.de
Garner JS, Emori WR, Horan TC, Hughes JM (1988) CDC definitions for nosocomial infections. Am J Infect Control 16: 128–140
Zuschneid I, Sohr D, Kohlhase C, Geffers C, Schumacher M, Gastmeier P, et al (2002) Accuracy of nosocomial infection data from intensive care units (ICUs) within the German Nosocomial Infection Surveillance System. In: Fifth International Conference of the Hospital Infection Society, 15.–18. 9. 2002. Edinburgh
Ehrenkranz NJ, Schulz JM, Richter EI (1995) Recorded criteria as a Gold standard for sensitivity and specificity estimates of surveillance of nosocomial infections. Infect Control Hosp Epidemiol 16: 697–702
Gastmeier P (2002) Nosokomiale Infektionen in der Intensivtherapie: Möglichkeiten und Grenzen eines Surveilance-Systems. Robert Koch-Institut, Berlin.
Keita-Perse O, Gaynes RP (1996) Severity of illness scoring systems to adjust nosocomial infection rates: a review and commentary. Am J Infect Control 24: 429–434
Soufir L, Timsit J-F, Mahe C, Carlet J, Regnier B, Chevret S (1999) Attributable morbidity and mortality of catheterrelated septicemia in critically ill patients: a matched. risk-adjusted, cohort study. Infect Control Hosp Epidemiol 20: 396–401
Weist K, Pollege K, Schulz I, Rüden H, Gastmeier P (2002) How many nosocomial infections are avoidable? A prospective cohort study in a surgical intensive care unit. Infect Control Hosp Epidemiol 23: 127–132
Hacek D, Suriano T, Noskin G, Kruszyski J, Reisberg B, Peterson L (1999) Medical and economical benefit of a comprehensive infection control program that includes routine determination of microbial clonality. Am J Clin Pathol 111: 647–654.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gastmeier, P., Geffers, C., Sohr, D. et al. Surveillance nosokomialer infektionen in intensivstationen: Aktuelle daten und Interpretationen. Wien Klin Wochenschr 115, 99–103 (2003). https://doi.org/10.1007/BF03040287
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03040287