
Abstract
Background
This retrospective analysis was performed in order to evaluate the pattern of relapse and the risk of late toxicity for solitary brain metastases treated with surgery and whole-brain radiotherapy and to correlate the results with those from radiosurgical trials.
Patients and Methods
From a total of 66 patients, 52 received 10×3 Gy and 10 were treated with 20×2 Gy whole-brain radiotherapy after resection of their brain metastases.
Results
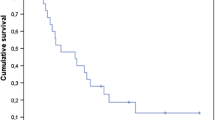
The actuarial probability of relapse was 27% and 55% after 1 and 2 year(s), respectively. The local relapse rate (at the original site of resected brain metastases) was rather high for melanoma, non-breast adenocarcinoma, and squamous-cell carcinoma. No local relapse occurred in breast cancer and small-cell carcinoma. Failure elsewhere in the brain seemed to be influenced by extracranial disease activity. Size of brain metastases and total dose showed no correlation with relapse rate. Occurrence of brain relapse was not associated with a reduced survival time, because 10/15 patients who developed a relapse received salvage therapy. Of the patients, 11 had symptoms of late radiation toxicity (the actuarial probability was 42% after 2 years).
Conclusions
Most results of surgical and radiosurgical studies are comparable to ours. Several randomized trials investigate surgical resection versus radiosurgery, as well as the effects of additional whole-brain radiotherapy in order to define the treatment of choice. Some data support the adjuvant application of 10×3 Gy over 2 weeks as a reasonable compromise when local control, toxicity, and treatment time have to be considered.
Zusammenfassung
Hintergrund
Das Rezidivmuster und die chronischen Strahlenspätfolgen nach Therapie solitärer Hirnmetastasen wurden retrospektiv ausgewertet. Die Behandlung bestand in einer Metastasenresektion und einer adjuvanten Ganzhirnbestrahlung. Die Ergebnisse wurden mit denen der Radiochirurgie verglichen.
Patientengut und Methode
Nach der Resektion der Hirnmetastase erhielten 52 von 66 Patienten eine Ganzhirnbestrahlung mit zehn Fraktionen von 3 Gy in zwei Wochen und zehn eine solche mit 20 Fraktionen von 2 Gy in vier Wochen.
Ergebnisse
Die Kaplan-Meier-Analyse ergab eine, Rezidivrate von insgesamt 27% nach einem bzw. 55% nach zwei Jahren. Rezidive im Bereich der resezierten Metastase wurden am häufigsten bei Melanomen, Adenokarzinomen (mit Ausnahme der Mammakarzinome) und Plattenepithelkarzinomen beobachtet. Dagegen traten bei Mammakarzinomen und kleinzelligen Karzinomen keine solchen Rezidive auf. Das Auftreten von Hirnmetastasen anderer Lokalisation schien vom Vorhandensein unkontrollierter extrakranieller Tumormanifestationen abhängig zu sein. Die Größe der Hirnfiliae und die Gesamtreferenzdosis der Strahlentherapie korrelierten nicht mit den Rezidivraten. Die Überlebenszeit der Patienten, die ein Rezidiv erlitten, unterschied sich nicht von der der anderen, da in zehn von 15 Rezidivfällen eine Salvagetherapie möglich war. Elf Patienten entwickelten chronische Strahlenspätfolgen. Nach Kaplan-Meier-Analyse betrug das Risiko 42% nach zwei Jahren.
Schlußfolgerungen
Die meisten Ergebnisse operativer und radiochirurgischer Studien sind den eigenen vergleichbar. Derzeit werden beide Verfahren in randomisierten Studien, miteinander verglichen. Auch die Effekte einer zusätzlichen Ganzhirnbestrahlung werden auf diese Weise untersucht. Unter Berücksichtigung der lokalen Kontrollrate, der Nebenwirkungen und der Behandlungszeit lassen einige Literaturangaben die adjuvante Applikation von zehnmal 3 Gy in zwei Wochen als vernünftigen Kompromiß erscheinen.
Similar content being viewed by others


References
Arbit E, Wronski M, Burt M, et al. The treatment of patients with recurrent brain metastases. Cancer 1995;76:765–773.
Armstrong JG, Wronski M, Galicich JH, et al. Postoperative radiation for lung cancer metastatic to the brain. J Clin Oncol 1994;12:2340–2344.
Auchter RM, Lamond JP, Alexander E, et al. A multiinstitutional outcome and prognostic factor analysis of radiosurgery for resectable brain metastasis. Int J Radiat Oncol Biol Phys 1996;35:27–35.
Bindal RK, Sawaya R, Laevens ME, et al. Reoperation for recurrent metastatic brain tumors. J Neurosurg 1995;84:442–448.
Flickinger JC, Kondziolka D, Lunsford LD, et al. A multi-institutional experience with stereotactic radiosurgery for solitary brain metastasis. Int J Radiat Oncol Biol Phys 1994;28:797–802.
Patchell RA, Tibbs PA, Walsh JW, et al. A randomized trial of surgery in the treatment of single metastases to the brain. N Engl J Med 1990;322:494–500.
Penar PL, Wilson JT. Cost and survival analysis of metastatic cerebral tumors treated by resection and radiation. Neurosurgery 1994;34:888–894.
Sause WT, Crowley JJ, Morantz R, et al. Results of an RTOG/SWOG protocol evaluation, surgery and radiation therapy versus radiation alone. Am J Clin Oncol 1990;13:427–432.
Shiau CY, Sneed PK, Shu HK, et al. Radiosurgery for brain metastases: relationship of dose and pattern of enhancement to local control. Int J Radiat Oncol Biol Phys 1997;37:375–383.
Shirato H, Takamura T, Tomita M, et al. Stereotactic irradiation without whole-brain irradiation for single brain metastasis. Int J Radiat Oncol Biol Phys 1997; 37:385–391.
Smalley SR, Schray MF, Laws ER, et al. Adjuvant radiation therapy after surgical resection of solitary brain metastasis: Association with pattern of failure and survival. Int J Radiat Oncol Biol Phys 1987;13:1611–1616.
Sundaresan N, Galicich JH. Surgical treatment of brain metastases. Cancer 1985;55:1382–1388.
Steel GG, ed. Basic clinical radiobiology. London: Edward Arnold, 1993: 72–79.
Vecht CJ, Haaxma-Reiche H, Noordijk EM, et al. Treatment of single brain metastases: radiotherapy alone or combined with neurosurgery? Ann Neurol 1993;33:583–590.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Nieder, C., Schwerdtfeger, K., Steudel, W.I. et al. Patterns of relapse and late toxicity after resection and whole-brain radiotherapy for solitary brain metastases. Strahlenther Onkol 174, 275–278 (1998). https://doi.org/10.1007/BF03038721
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03038721