
Abstract
Purpose
At present, there are no guidelines and insufficient evidence to guide the decision-making of anesthesiologists in the perioperative care of patients with obstructive sleep apnea (OSA). The purpose of this study was to examine the current perioperative care provided, and to obtain opinions from anesthesiologists regarding evidence/consensus based guidelines to assist them in providing care to patients with OSA.
Methods
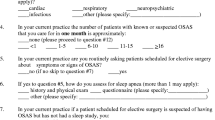
Canadian anesthesiologists were sent a postal questionnaire examining their opinions and perioperative care of patients with OSA. Respondents were asked to indicate the postoperative monitoring they would most likely select for two clinical scenarios, representing administration of a general and regional anesthetic, which was altered to reflect: treatment of OSA; use of postoperative opioids; presence of morbid obesity; and increased severity of OSA.
Results
The survey had a response rate of 70% (746/1,063). Sixty-seven percent of respondents provided perioperative care to one to five patients with OSA per month, and 72% reported not having departmental policies for care of OSA patients. Ninety-two percent reported asking patients about OSA preoperatively. There was ≥ 75% respondent agreement in two of the five alterations of the general anesthesia case scenario and in none of the alterations of the regional anesthesia case scenario. Eighty-two percent reported that guidelines would assist them in caring for patients with OSA.
Conclusion
This study demonstrates a variation amongst anesthesiologists in their postoperative monitoring of patients with OSA. The majority surveyed do not have departmental policies, and believed that guidelines would assist them in providing care to patients with OSA.
Résumé
Objectif
Actuellement, les lignes directrices sont absentes et la preuve insuffisante pour guider les anesthésiologistes dans la prise en charge périopératoire des patients atteints ďapnée du sommeil ďorigine obstructive (ASO). Notre but était ďexaminer la démarche périopératoire actuelle et de sonder les anesthésiologistes sur des directives fondées sur la preuve/un consensus pour les assister auprés de ces patients.
Méthode
Un questionnaire postal a été envoyé aux anesthésiologistes canadiens à cet effet. Les répondants devaient indiquer quel monitorage postopératoire ils choisiraient selon deux scénarios cliniques représentant ľadministration ďune anesthésie générale et régionale et modifiés pour illustrer: le traitement de ľASO, ľusage ďopioïdes postopératoires, la présence ďobésité morbide et la sévérité croissante ďASO.
Résultats
Le taux de réponse a été de 70 % (746/1 063). Parmi les répondants, 67 % donnaient des soins périopératoires à un patient sur cinq, par mois, atteint ďASO et 72 % mentionnaient ľabsence de politique départementale sur ľASO. Quatrevingt-douze pour cent interrogeaient leur patient sur ľASO avant ľopération. Il y a eu une concordance de ≥ 75 % pour deux modifications sur cinq du scénario de ľanesthésie générale et pour une des modifications du scénario de ľanesthésie régionale. Quatrevingt-deux pour cent ont rapporté que des directives les aideraient à traiter les patients atteints ďASO.
Conclusion
Ľétude démontre des variations dans le monitorage postopératoire des patients atteints ďASO, réalisé par les anesthésiologistes. La majorité des répondants a rapporté ľabsence de politique départementale et croit que des directives faciliteraient le traitement de ľASO.
Similar content being viewed by others


References
Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Eng J Med 1993; 328: 1230–5.
Benumof JL. Policies and procedures needed for sleep apnea patient (Letter). Anesthesia Patient Safety Foundation Newsletter 2002; 17: 57.
Dillman DA. Mail and Internet Surveys. The Tailored Design Method, 2nd ed. New York: John Wiley & Sons; 2000.
Davies S, Cleave-Hogg D. Continuing medical education should be offered by both e-mail and regular mail: a survey of Ontario anesthesiologists. Can J Anesth 2004; 51: 444–8.
VanDenKerkhof EG, Milne B, Parlow JL. Knowledge and practice regarding prophylactic perioperative beta blockade in patients undergoing noncardiac surgery: a survey of Canadian anesthesiologists. Anesth Analg 2003; 96: 1558–65.
Deutscher R, Bell D, Sharma S. OSA protocol promotes safer care (Letter). Anesthesia Patient Safety Foundation Newsletter 2002; 17: 58.
Loadsman JA, Hillman DR. Anaesthesia and sleep apnoea. Br J Anaesth 2001; 86: 254–66.
Meoli AL, Rosen CL, Kristo D, et al;Clinical Practice Review Committee; American Academy of Sleep Medicine. Upper airway management of the adult patient with obstructive sleep apnea in the perioperative period-Avoiding complications. Sleep 2003; 26: 1060–5.
Emerson BM, Wrigley SR, Newton M. Pre-operative fasting for paediatric anaesthesia. A survey of current practice. Anaesthesia 1998; 53: 326–30.
Jacka MJ, Cohen MM, To T, Devitt JH, Byrick R. The appropriateness of the pulmonary artery catheter in cardiovascular surgery. Can J Anesth 2002; 49: 276–82.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Rights and permissions
About this article
Cite this article
Turner, K., VanDenKerkhof, E., Lam, M. et al. Perioperative care of patients with obstructive sleep apnea — a survey of Canadian anesthesiologists. Can J Anesth 53, 299–304 (2006). https://doi.org/10.1007/BF03022219
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03022219