
Abstract
Purpose
In order to minimize the potential for dental damage and to improve laryngeal visualization during tracheal intubation, two commonly used laryngoscope blades were modified and compared in a clinical setting: the Miller laryngoscope blade and the Macintosh laryngoscope blade. Modified versions of both laryngoscope blades with a lowered heel (Callander modification) at the proximal end of the blade were compared to standard blades.
Methods
Forty patients scheduled for general anesthesia requiring endotracheal intubation were studied prospectively. Preoperatively, the patients’ airways were evaluated according to Mallampati score, thyromental distance and interincisor gap. After induction of anesthesia laryngoscopy was performed with the original laryngoscope and its modified counterpart in random order. A lateral x-ray of the neck was taken after the optimal view had been obtained, and blade-tooth distance, laryngeal view, blade-tooth contact and need for assistance were measured. Using angular calculations the laryngoscopes were analyzed at different insertion depths on graph paper, and the results were compared with data from the lateral x-rays.
Results
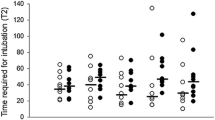
With a modified Macintosh blade the blade-tooth distance was significantly greater in comparison to the original design (2.5 ± 2.1 cmvs 0.2 ± 0.1 cm,P < 0.01). Consequently the number of blade-tooth contacts was significantly lower (20%vs 75%,P < 0.05). The best laryngeal view could be obtained using a modified Macintosh laryngoscope. With a modified Miller laryngoscope laryngeal visibility was not improved and assistance was required more often to achieve adequate intubating conditions (35%vs 5%,P < 0.05).
Conclusion
A reduction of the proximal flange of a Miller blade decreases the blade’s effectiveness for laryngeal visualization, whereas a similar modification of a Macintosh blade increases blade-tooth distance, decreases the number of blade tooth contacts and provides a better laryngeal view.
Résumé
Objectif
Pour réduire le risque de dommage aux dents et pour améliorer la visualisation du larynx pendant ľintubation endotrachéale, deux lames de laryngoscope fréquemment utilisées ont été modifiées et comparées en situation clinique, celles des laryngoscopes Miller et Macintosh. Les versions modifiées des deux lames, munies ďun talon plus bas à ľextrémité proximale (modification Callander), ont été comparées aux lames régulières.
Méthode
Quarante patients devant subir une anesthésie générale avec intubation endotrachéale ont fait ľobjet ďune étude prospective. Ľévaluation préopératoire des voies respiratoires selon le score de Mallampati a révélé la distance thyromentonnière et ľespace interincisive. Après ľinduction de ľanesthésie, la laryngoscopie a été réalisée avec le laryngoscope original et sa version modifiée suivant un ordre aléatoire. Une fois la vision optimale obtenue, une radiographie latérale du cou a été prise, puis la distance entre la lame et les dents, la vision laryngée, la présence de contact entre la lame et les dents et la nécessité ďune assistance ont été évaluées. D’après le calcul des angles, une analyse graphique des laryngoscopes a été faite pour différentes profondeurs ďinsertion et les résultats comparés avec les données de la radiographie latérale.
Résultats
Avec la lame Macintosh modifiée, la distance dentlame a été significativement plus grande qu’avec la lame originale (2,5 ± 2,1 cm vs 0,2 ± 0,1 cm, P < 0,01). Le nombre de contacts dent-lame a donc été significativement plus bas (20 % vs 75 %, P < 0,05). La meilleure vision laryngée a pu être obtenue avec une lame Macintosh modifiée. Avec le laryngoscope Miller modifié, la visibilité du larynx n’était pas améliorée et une assistance a été plus souvent requise pour atteindre des conditions ďintubation adéquates (35 % vs 5 %, P < 0,05).
Conclusion
Une réduction du manche proximal de la lame Miller diminue la qualité de la visualisation laryngée obtenue tandis qu’une modification similaire de la lame Macintosh améliore la distance dent-lame, diminue le nombre de contacts dent-lame et fournit une meilleure vision du larynx.
Article PDF
Similar content being viewed by others


References
Cooper SD. The evolution of upper airway retraction: new and old laryngoscope blades.In: Benumof JL (Ed.). Airway Management. Principles and Practice, 1st ed. St. Louis, MO: Mosby; 1996: 374–411.
Dorsch JE, Dorsch SE. Laryngoscopes.In: Dorsch JE, Dosch SE (Eds). Understanding Anesthesia Equipment, 3rd ed. Baltimore: Williams and Wilkins; 1984: 399–437.
Cooper SD. Laryngoscope blades and lighted stylets.In: Hanowell LH, Waldron RJ, Hwang JCF (Eds). Airway Management, 1st ed. Philadelphia: Lippincott-Raven; 1996: 223–57.
Owen H, Waddell-Smith I. Dental trauma associated with anaesthesia. Anaesth Intensive Care 2000; 28: 133–45.
Warner ME, Benenfeld SM, Warner MA, Schroeder DR, Maxson PM. Perianesthetic dental injuries: frequency, outcomes and risk factors. Anesthesiology 1999; 90: 1302–5.
Bizzarri DV, Giuffrida JG. Improved laryngoscope blade designed for ease of manipulation and reduction of trauma. Anesth Analg 1985; 37: 231–2
Ibler M. Modification of Macintosh laryngoscope blade. Anesthesiology 1983; 58: 200–1.
Callander CC, Thomas J. Modification of Macintosh laryngoscope for difficult intubtion. Anesthesia 1987; 42: 671–2.
Bucx MJ, Snijders CJ, ven der Vegt MH, Holstein JD, Stijnen T. Reshaping the Macintosh blade using biomechanical modelling. A prospective comparative study in patients. Anaesthesia 1997; 52: 662–7.
Marks RR, Hancock R, Charters P. An analysis of laryngoscope blade shape and design: new criteria for laryngoscope evaluation. Can J Anaesth 1993; 40: 262–70.
Lee J, Choi JH, LeeYK, Kim ES, Kwon OK, Hastings RH. The Callander laryngoscope blade modification is associated with a decreased risk of dental contact. Can J Anesth 2004; 51: 181–4.
Watanabe S, Suga A, Asakura N, et al. Determination of the distance between the laryngoscope blade and the upper incisors during direct laryngoscopy: comparisons of a curved, an angulated straight, and two straight blades. Anesth Analg 1994; 79: 638–41.
Maleck WH, Koetter KP, Lenz M, Piper SN, Triem J, Boldt J. A randomised comparison of three laryngoscopes with the Macintosh. Resuscitation 1999; 42: 241–5.
Papageorgiou E, Kokkinis K, Goumas P, Mochloulis G, Alexopoulos C. Objective evaluation of the difficulty of endotracheal intubation. A comparative study of two different laryngoscope blades. Anaesth Intensive Care 1997; 25: 655–8.
Lockhart PB, Feldbau EV, Gabel RA, Connolly SF, Silversin JB. Dental complications during and after tracheal intubation. J Am Dent Assoc 1986; 112: 480–3.
Yardeni IZ, Gefen A, Smolyarenko V, Zeidel A, Beilin B. Design evaluation of commonly used rigid and levering laryngoscope blades. Acta Anaesthesiol Scand 2002; 46: 1003–9.
Nakahashi K, Yamamoto K, Tsuzuki M, et al. Effect of teeth protector on dental injuries during general anesthesia (Japanese). Masui 2003; 52: 26–31.
Bellhouse CP. An angulated laryngoscope for routine and difficult tracheal intubation. Anesthesiology 1988; 69: 126–9.
Arino JJ, Velasco JM, Gasco C, Lopez-Timoneda F. Straight blades improve visualization of the larynx while curved blades increase ease of intubation: a comparison of the Macintosh, Miller, McCoy, Belscope and Lee-Fiberview blades. Can J Anesth 2003; 50: 501–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kimberger, O., Fischer, L., Plank, C. et al. Lower flange modification improves performance of the Macintosh, but not the Miller laryngoscope blade. Can J Anesth 53, 595–601 (2006). https://doi.org/10.1007/BF03021851
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03021851