
Abstract
Purpose
Paraplegia is an uncommon yet devastating complication following thoracotomy, usually caused by compression or ischemia of the spinal cord. Ischemia without compression may be a result of global ischemia, vascular injury and other causes. Epidural anesthesia has been implicated as a major cause. This report highlights the fact that perioperative cord ischemia and paraplegia may be unrelated to epidural intervention.
Clinical features
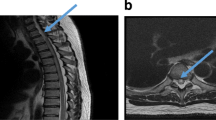
A 71-yr-old woman was admitted for a left upper lobectomy for resection of a non-small cell carcinoma of the lung. The patient refused epidural catheter placement and underwent a left T5–6 thoracotomy under general anesthesia. During surgery, she was hemodynamically stable and good oxygen saturation was maintained. Several hours following surgery the patient complained of loss of sensation in her legs. Neurological examination disclosed a complete motor and sensory block at the T5–6 level. Magnetic resonance imaging (MRI) revealed spinal cord ischemia. The patient receivediv steroid treatment, but remained paraplegic. Five months following the surgery there was only partial improvement in her motor symptoms. A follow-up MRI study was consistent with a diagnosis of spinal cord ischemia.
Conclusion
In this case of paraplegia following thoracic surgery for lung resection, epidural anesthesia/analgesia was not used. The MRI demonstrated evidence of spinal cord ischemia, and no evidence of cord compression. This case highlights that etiologies other than epidural intervention, such as injury to the spinal segmental arteries during thoracotomy, should be considered as potential causes of cord ischemia and resultant paraplegia in this surgical population.
Résumé
Objectif
La paraplégie est une complication rare mais dévastatrice de la thoracotomie, causée habituellement par la compression ou ľischémie de la moelle épinière. Ľischémie sans compression peut résulter de causes diverses dont une ischémie générale ou une lésion vasculaire. Alors que ľanesthésie péridurale est vue comme cause majeure, notre article souligne que ľischémie médullaire périopératoire et la paraplégie n’y sont peut-être pas reliées.
Éléments cliniques
Une femme de 71 ans a subi une lobectomie supérieure gauche pour la résection ďun carcinome pulmonaire non à petites cellules. Elle a refusé la mise en place ďun cathéter péridural et a subi une thoracotomie en T5–6 sous anesthésie générale. Pendant ľopération, ľhémodynamique a été stable et une bonne saturation du sang en oxygène a été maintenue. Quelques heures après ľopération, la patiente a éprouvé une perte de sensibilité aux jambes. Ľexamen neurologique a révélé un bloc moteur et sensitif complet débutant à T5–6. Ľimagerie par résonance magnétique (IRM) a montré une ischémie de la moelle épinière. La patiente a reçu un traitement stéroïde iv, mais est demeurée paraplégique. Cinq mois après ľopération, il n’y avait qu’une amélioration partielle des symptômes moteurs. Un examen ďIRM de contrôle confirmait le diagnostic ďischémie de la moelle épinière.
Conclusion
Dans ce cas de paraplégie suivant une thoracotomie pour résection pulmonaire, ni ľanesthésie ni ľanalgésie péridurales n’ont été utilisées. ĽIRM a prouvé une ischémie de la moelle épinière et ľabsence de compression médullaire. D’autres causes, comme la lésion des artères rachidiennes segmentaires pendant la thoracotomie, doivent être jugées susceptible de provoquer une ischémie médullaire suivie ďune paraplégie dans cette population chirurgicale.
Article PDF
Similar content being viewed by others


References
Kane RE. Neurologic deficits following epidural or spinal anesthesia. Anesth Analg 1981; 60: 150–61.
Attar S, Hankins JR, Turney SZ, Krasna MJ, McLaughlin JS. Paraplegia after thoracotomy: report of five cases and review of the literature. Ann Thorac Surg 1995; 59: 1410–5; discussion 1415-6.
Popat KU, Ngyugen T, Kowalski AM, Daley MD, Arens JF, Thakar D. Postoperative paraplegia after nonvascular thoracic surgery. Internet J Anesthesiol 2004; 8: 1.
Lovstad RZ, Steen PA, Forsman M. Paraplegia after thoracotomy-not caused by the epidural catheter. Acta Anaesthesiol Scand 1999; 43: 230–2.
Wada E, Yonenobu K, Ebara S, Kuwahara O, Ono K. Epidural migration of hemostatic agents as a cause of postthoracotomy paraplegia. Report of two cases. J Neurosurg 1993; 78: 658–60.
Dogan S, Kocaeli H, Doygun M. Oxidised regenerated cellulose as a cause of paraplegia after thoracotomy: case report and review of the literature. Spinal Cord 2005; 43: 445–7.
Iwabuchi S, Koike K, Okabe T, Tago S, Murakami T. Iatrogenic paraplegia caused by surgicel used for hemostasis during a thoracotomy: report of a case. Surg Today 1997; 27: 969–70.
Wulf H. Epidural anaesthesia and spinal haematoma. Can J Anaesth 1996; 43: 1260–71.
Cheshire WP, Santos CC, Massey EW, Howard JF Jr. Spinal cord infarction: etiology and outcome. Neurology 1996; 47: 321–30.
Bhuiyan MS, Mallick A, Parsloe M. Post-thoracotomy paraplegia coincident with epidural anaesthesia. Anaesthesia 1998; 53: 583–6.
Massad MG, Donahue PE, Rubeiz H, et al. Paraplegia after esophagectomy: who are the patients at risk? J Thorac Cardiovasc Surg 2001; 121: 386–8.
Brewer LA III, Fosburg RG, Mulder GA, Verska JJ. Spinal cord complications following surgery for coarctation of the aorta. A study of 66 cases. J Thorac Cardiovasc Surg 1972; 64: 368–81.
Konstantinidou AS, Balamoutsos NG. Paraplegia in a patient who by chance missed the insertion of an epidural catheter (Letter). Anesth Analg 1996; 82: 1110.
Bromage PR. Paraplegia in a patient who by chance missed the insertion of an epidural catheter (Letter). Anesth Analg 1996; 83: 1351.
Urquhart-Hay D. Paraplegia following epidural analgesia. Anaesthesia 1969; 24: 461–70.
Chan LL, Kumar AJ, Leeds NE, Forman AD. Post-epidural analgesia spinal cord infarction: MRI correlation. Acta Neurol Scand 2002; 105: 344–8.
Wan IY, Angelini GD, Bryan AJ, Ryder I, Underwood MJ. Prevention of spinal cord ischaemia during descending thoracic and thoracoabdominal aortic surgery. Eur J Cardiothorac Surg 2001; 19: 203–13.
Blacker DJ, Wijdicks EF, Ramakrishna G. Resolution of severe paraplegia due to aortic dissection after CSF drainage. Neurology 2003; 61: 142–3.
Tiesenhausen K, Amann W, Koch G, Hausegger KA, Oberwalder P, Rigler B. Cerebrospinal fluid drainage to reverse paraplegia after endovascular thoracic aortic aneurysm repair. J Endovasc Ther 2000; 7: 132–5.
Hall ED, Springer JE. Neuroprotection and acute spinal cord injury: a reappraisal. NeuroRx 2004; 1: 80–100.
Skouen JS, Wainapel SF, Willock MM. Paraplegia following epidural anesthesia. A case report and a literature review. Acta Neurol Scand 1985; 72: 437–43.
Shamji MF, Maziak DE, Shamji FM, Ginsberg RJ, Pon R. Circulation of the spinal cord: an important consideration for thoracic surgeons. Ann Thorac Surg 2003; 76: 315–21.
Thron AK. Vascular Anatomy of the Spinal Cord — Neuroradiological Investigations and Clinical Syndromes. New York: Springer-Verlag; 1988.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Raz, A., Avramovich, A., Saraf-Lavi, E. et al. Spinal cord ischemia following thoracotomy without epidural anesthesia. Can J Anesth 53, 551–555 (2006). https://doi.org/10.1007/BF03021844
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03021844