
Abstract
Purpose
In previous animal studies, a prior exposure to nonsteroidal anti-inflammatory drugs (NSAID) augmented opioid drug potency. This study was designed to answer the question whether a similar effect can be attained in man. The objective was to use NSAID for preoperative pain reduction and at the same time use the NSAID exposure to reduce opioid requirements for pain inhibition in major orthopedic surgery.
Methods
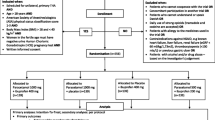
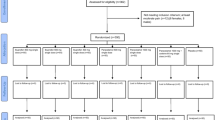
In this double-blind, randomized study, 50 patients scheduled for total hip surgery were included. Patients of Group I received a placebo drug three times a day two weeks before surgery, and those allocated to Group II received ibuprofen (600 mg) three times a day. For surgical anesthesia, all patients received intrathecal bupivacaine 20 mg plus 0.1 mg morphine in a total volume of 4 mL.
Results
The preoperative or postoperative visual analogue scale pain scores or the amount of iv morphine showed no differences between the two groups in the first 24 hr after surgery. The median total blood loss in the ibuprofen group was 1161 mL vs 796 mL in the placebo group (P < 0.01).
Conclusion
Pretreatment with ibuprofen before major hip surgery does not improve the pain scores or reduce morphine requirement but significantly increases blood loss. Considering the presence of relevant adverse effects, pretreatment with a nonselective NSAID is not recommended.
Résumé
Objectif
Des études antérieures sur des animaux ont démontré qu’une exposition préalable aux anti-inflammatoires non stéroidiens (AINS) renforce l’effet des opiacés. Cette étude a été conçue pour savoir si le même effet peut être obtenu chez l’homme. L’objectif était de prescrire un traitement antalgique préopératoire aux AINS et en même temps, profitant de l’exposition aux AINS, de réduire le besoin d’opiacés pour diminuer la douleur après des opérations orthopédiques majeures.
Méthode
Cinquante patients opérés pour la mise en place d’une prothèse totale de la hanche ont été inclus dans cette étude randomisée et en double aveugle. Les patients du Groupe I prenaient un placebo trois fois par jour pendant deux semaines avant l’opération tandis que les patients du Groupe Il prenaient de l’ibuprofène (600 mg) trois fois par jour. L’anesthésie pratiquée à l’ensemble des patients consistait en l’injection intrathécale de 20 mg de bupivacaïne et 0,1 mg de morphine dans un volume total de 4 mL.
Résultats
Aucune différence n’a été constatée entre les deux groupes dans les degrés de douleur mesurée par échelle visuelle analogique aussi bien en préopératoire qu’en postopératoire ou dans la dose de morphine injectée par voie iv pendant les 24 premières heures après l’opération. La perte totale de sang dans le groupe ibuprofène s’élevait à I 161 mL et dans le groupe placebo à 796 mL.
Conclusion
Un traitement préalable à l’ibuprofène en chirurgie majeure de la hanche n’améliore pas la douleur et ne diminue pas le besoin de morphine postopératoire, mais est associé avec une perte de sang signifcativement plus élevée. Vu ces conséquences fâcheuses, il nous apparaît judicieux de s’abstenir d’un traitement préalable aux AINS non sélectifs avant ce type de chirurgie.
Article PDF
Similar content being viewed by others

References
Yaksh TL, Jessell TM, Gamse R, Mudge AW, Leeman SE. Intrathecal morphine inhibits substance P release from mammalian spinal cord in vivo. Nature 1980; 286: 155–7.
Malmberg AB, Yaksh TL. Spinal actions of nonsteroidal anti-inflammatory drugs: evidence for a central role of prostanoids in nociceptive processing. Prog Pharmacol Clin Pharmacol 1993; 10: 91–110.
McCormack K. Non-steroidal anti-inflammatory drugs and spinal nociceptive processing. Pain 1994; 59: 9–43.
Malmberg AB, Yaksh TL. Hyperalgesia mediated by spinal glutamate or substance P receptor blocked by spinal cyclooxygenase inhibition. Science 1992; 257: 1276–9.
Trujillo KA, Akil H. Inhibition of morphine tolerance and dependence by the NMDA receptor antagonist MK-801. Science 1991; 251: 85–7.
Mao J, Price DD, Mayer DJ. Thermal hyperalgesia in association with the development of morphine tolerance in rats: roles of excitatory amino acid receptors and protein kinase C. J Neurosci 1994; 14: 2301–12.
Tiseo PJ, Inturrisi CE. Attenuation and reversal of morphine tolerance by the competitive N-methyl-D-aspartate receptor antagonist, LY274614. J Pharmacol Exp Ther 1993; 264: 1090–6.
Dunbar S, Yaksh TL. Concurrent spinal infusion of MK801 blocks spinal tolerance and dependence induced by chronic intrathecal morphine in the rat. Anesthesiology 1996; 84: 1177–88.
Shimoyama N, Shimoyama M, Lnturrisi CE, Elliott KJ. Ketamine attenuates and reverses morphine tolerance in rodents. Anesthesiology 1996; 85: 1357–66.
Powell KJ, Hosokawa A, Bell A, et al. Comparative effects of cyclo-oxygenase and nitric oxide synthase inhibition on the development and reversal of spinal opioid tolerance. Br J Pharmacol 1999; 127: 631–44.
Eukuda IC, Kato S, Morikawa H, Shoda T, Mori K. Functional coupling of the δ-, μ-, and κ-opioid receptors to mitogen-activated protein kinase and arachidonate release in Chinese hamster ovary cells. J Neurochem 1996; 67: 1309–16.
Matsumura K, Watanabe Y, Lmai-Matsumura K, et al. Mapping of prostaglandin E2 binding sites in rat brain using quantitative autoradiography. Brain Res 1992; 581:292–8.
Nicol GD, Klingberg DK, Vasko MR. Prostaglandin E2 increases calcium conductance and stimulates release of substance P in avian sensory neurons. J Neurosci 1992; 12: 1917–27.
Slappendel R, Weber EWG, Bugter MLT, Dirksen R. The intensity of preoperative pain is directly correlated with the amount of morphine needed for postoperative analgesia. Anesth Analg 1999; 88: 146–8.
Eournier R, Van Gessel E, Macksay M, Gamulin Z. Onset and offset of intrathecal morphine versus nalbuphine for postoperative pain relief after total hip replacement. Acta Anaesthesiol Scand 2000; 44: 940–5.
Fournier R, Van Gessel E, Weber A, Gamulin Z. A comparison of intrathecal analgesia with fentanyl or sufentanil after total hip replacement. Anesth Analg 2000; 90: 918–22.
Slappendel R, Weber EWG, Dirksen R, Gielen MJM, van Limbeek J. Optimization of the dose of intrathecal morphine in total hip surgery: a dose-finding study. Anesth Analg 1999; 88: 822–6.
Carpenter RL, Caplan RA, Brown DL, Stephenson C, Wu R. Incidence and risk factors for side effects of spinal anesthesia. Anesthesiology 1992; 76: 906–16.
Fletcher D, Zetlaoui P, Monin S, Bombart M, Samii K. Influence of timing on the analgesic effect of intravenous ketorolac after orthopedic surgery. Pain 1995; 61:291–7.
Kissin I. Preemptive analgesia. Anesthesiology 2000; 93: 1138–43.
Schafer AI. Effects of nonsteroidal antiinflammatory drugs on platelet function and systemic hemostasis. J Clin Pharmacol 1995; 35: 209–19.
Rorarius MGF, Baer GA, Metsa-Ketala T, Miralles J, Palomaki E, Vapaatalo H. Effects of peri-operatively administered diclofenac and indomethacin on blood loss, bleeding time and plasma prostanoids in man. Eur J Anaesth 1989;6: 335–42.
Vane JR, Botting RM. Pharmacodynamic profile of prostacyclin. Am J Cardiol 1995; 75: 3A-10A.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bugter, M.L.T., Dirksen, R., Jhamandas, K. et al. Prior ibuprofen exposure does not augment opioid drug potency or modify opioid requirements for pain inhibition in total hip surgery. Can J Anesth 50, 445–449 (2003). https://doi.org/10.1007/BF03021054
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03021054