
Abstract
Purpose
To compare, over a 48-hr follow-up period, the analgesia and side-effects of patient controilediv analgesia (PCA) with morphine alonevs combined intrathecal and PCA morphine (IT+PCA) in patients undergoing major abdominal surgery.
Methods
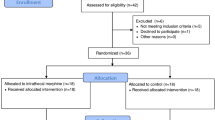
Sixty adult patients undergoing abdominal surgery for cancer were randomly allocated to receive preoperative IT (0,3 or 0,4 mg) plus postoperative PCA morphine or postoperative PCA morphine alone. Postoperative analgesia was tested at rest and while coughing on a visual analogue pain scale and morphine consumption was recorded. Patients’ satisfaction, arterial oxygen saturation, respiratory rate, episodes of nausea, vomiting and pruritus were also noted.
Results
Analgesia at rest and while coughing was significantly better in the IT+PCA morphine group (rest:P = 0,01; coughing:P = 0,005) on the first postoperative day only, IT+PCA morphine constantly provided adequate analgesia during this period. Morphine consumption was lower in the IT+PCA morphine group during this period also (IT+PCA: 9 (17)vs PCA: 40 (26); mg of morphine, mean (SD),P = 0,0001), No difference was found in pain relief and morphine consumption between the groups on the second postoperative day. Nausea and vomiting were more frequent with IT+PCA morphine on the first postoperative day. No respiratory depression occurred in either group. Satisfaction was high in both groups.
Conclusions
IT+PCA morphine improves patient comfort constantly during the first postoperative day after major abdominal surgery. However, after the first postoperative day, IT+PCA morphine provides no additional benefit.
Résumé
Objectif
Comparer, pendant un suivi de 48 h, l’anaigésie et les effets secondaires de l’anaigésie iv auto- contrôlée (AAC) avec de la morphine seule vs de la morphine en AAC combinée à de la morphine intrathécale (IT+AAC) chez des patients qui subissent une intervention chirurgicale abdominale majeure.
Méthode
Soixante patients adultes devant subir une intervention abdominale pour un cancer ont été répartis au hasard et ont reçu de la morphine IT préopératoire (0,3 ou 0,4 mg) plus de la morphine postopératoire en AAC ou seulement de la morphine postopératoire en AAC. Lanalgésie postopératoire a été testée au repos et pendant la toux au moyen d’une échelle visuelle analogique. Aussi, on a noté la consommation de morphine, la satisfaction des patients, la saturation de sang en oxygène, le rythme respiratoire, les nausées, les vomissements et le prurit.
Résultats
Lanalgésie au repos et pendant la toux a été significativement meilleure dans le groupe IT+AAC (repos: P = 0,01; toux: P = 0,005) au premier jour postopératoire seulement. La morphine IT+AAC a fourni régulièrement une analgésie adéquate pendant cette période. La consommation de morphine a été plus faible dans le groupe IT+AAC pendant ce même temps (IT+AAC: 9 (17) vs AAC: 40 (26); tmg de morphine, moyenne (écart type) P = 0,0001). Aucune différence d’analgésie et de consommation de morphine intergroupes n’a été trouvée le deuxième jour postopératoire. Les nausées et les vomissements ont été plus fréquents avec la morphine IT+AAC au premier jour postopératoire. Aucune dépression respiratoire n’a été enregistrée. La satisfaction a été élevée chez les patients des deux groupes.
Conclusion
La morphine IT+AAC améliore le confort du patient de façon constante pendant le premier jour postopératoire suivant une opération abdominale majeure. Cependant, par la suite, la morphine IT+AAC ne donne plus d’avantage supplémentaire.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Abboud TIC, Dror A, Mosaad P, et al. Mini-dose intrathecal morphine for the relief of post-cesarean section pain: safety, efficacy, and ventilatory responses to carbon dioxide. Anesth Analg 1988; 67: 137–43.
Motamed C, Bouaziz H, Franco D, Benhamou D. Analgesic effect of low-dose intrathecal morphine and bupivacaine in laparoscopic cholecystectomy. Anaesthesia 2000; 55: 118–24.
Surma VJ, Bostrom UV. Intrathecal morphine for the relief of post-hysterectomy pain-a double-blind, dose-response study. Acta Anaesthesiol Scand 1993; 37: 223–7.
Gray JR, Fromme GA, Nauss LA., Wang JK, Itstrup DM. Intrathecal morphine for post-thoracotomy pain. Anesth Analg 1986; 65: 873–6.
France JC, Jorgenson SS, Lowe TG, Dwyer AP. The use of intrathecal morphine for analgesia after posterolateral lumbar fusion. A prospective, double-blind, randomized study. Spine 1997; 22: 2272–7.
Fogarty DJ, Carabine UA, Milligan KR. Comparison of the analgesic effects of intrathecal clonidine and intrathecal morphine after spinal anaesthesia in patients undergoing total hip replacement. Br J Anaesth 1993; 71: 661–4.
Gall O, Aubineau JV, Berniere J, Desjeux L, Murat I. Analgesic effect of low-dose intrathecal morphine after spinal fusion in children. Anesthesiology 2001; 94: 447–52.
Mason N, Gondret R, Junca A, Bonnet F. Intrathecal sufentanil and morphine for post-thoracotomy pain relief. Br J Anaesth 2001; 86: 236–40.
Macintyre PE. Safety and efficacy of patient-controlled analgesia. Br J Anaesth 2001; 87: 36–46.
Aubry P, Jounieaux V, Rose D, Duran A, Levi-Valensi P. The SaO2/t diagram as a useful means to express nocturnal hypoxemia. Chest 1989; 96: 1341–5.
Swart M, Sewell J, Thomas D. Intrathecal morphine for caesarean section: an assessment of pain relief, satisfaction and side-effects. Anaesthesia 1997; 52: 373–81.
McCoy EP, Furness G, Wright PM. Patient-controlled analgesia with and without background infusion. Analgesia assessed using the demand: delivery ratio. Anaesthesia 1993; 48: 256–65.
Jayr C, Beaussier M, Gustafison U, et al. Continuous epidural infusion of ropivacaine for postoperative analgesia after major abdominal surgery: comparative study with i.v. PCA morphine. Br J Anaesth 1998; 81: 887–92.
Gwirtz KH, Young JV, Byers RS, et al. The safety and efficacy of intrathecal opioid analgesia for acute postoperative pain: seven years’ experience with 5969 surgical patients at Indiana University Hospital. Anesth Analg 1999; 88: 599–604.
Rawal N, Arner S, Gustafsson LL, Allvin R. Present state of extradural and intrathecal opioid analgesia in Sweden. Br J Anaesth 1987; 59: 791–9.
Abouleish E, Rawal N, Rashad MN. The addition of 0.2 mg subarachnoid morphine to hyperbaric bupivacaine for cesarean delivery: a prospective study of 856 cases. Reg Anesth 1991; 16: 137–40.
Taksh TL. Pharmacology and mechanisms of opioid analgesic activity.In: Yaksh TL, Lynch CL, Zapol WM, Maze M, Biebuyck JF, Saidman LJ (Eds.). Anesthesia: Biologic Foundations. Philadelphia: Lippincott-Raven; 1997: 921–35.
Ready LB, Oden R, Chadwick HS, et al. Development of an anesthesiology-based postoperative pain management service. Anesthesiology 1988; 68: 100–6.
Clergue F, Montembault C, Despierres O, Ghesquiere F, Harari A, Viars P. Respiratory effects of intrathecal morphine after upper abdominal surgery. Anesthesiology 1984; 61: 677–85.
Glass PSA. Respiratory depression following only 0.4 mg of intrathecal morphine (Letter). Anesthesiology 1984; 60: 256–7.
Bailey PL, Lu JK, Pace NL, et al. Effects of intrathecal morphine on the ventilatory response to hypoxia. N Engl J Med 2000; 343: 1228–34.
Bailey PL, Rhondeau S, Schafer PG, et al. Dose-response pharmacology of intrathecal morphine in human volunteers. Anesthesiology 1993; 79: 49–59.
Cousins MJ, Mather LE. Intrathecal and epidural administration of opioids. Anesthesiology 1984; 61: 276–310.
Pitkanen MT, Niemi L, Tuominen MK, Rosenberg PH. Effect of tropisetron, a 5-HT3-receptor antagonist, on analgesia and nausea after intrathecal morphine. Br J Anaesth 1993; 71: 681–4.
Lydon AM, Cooke T, Duggan F, Shorten GD. Delayed postoperative gastric emptying following intrathecal morphine and intrathecal bupivacaine. Can J Anesth 1999; 46: 544–9.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work should be attributed to the Department of Anaesthesiology, Gustave Roussy Institute, 39 Rue Camille Desmoulins, 94805 Villejuif Cedex, France.
Rights and permissions
About this article
Cite this article
Devys, JM., Mora, A., Plaud, B. et al. Intrathecal + PCA morphine improves analgesia during the first 24 hr after major abdominal surgery compared to PCA alone. Can J Anesth 50, 355–361 (2003). https://doi.org/10.1007/BF03021032
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03021032