
Abstract
Purpose
To describe the development and performance of a new minimal contact oxygen (O2) delivery system for both nasal and oral breathing, with capnographic capabilities.
Methods
The development and design challenges of the OxyArm™ (OA) prototype are described. The innovative design utilizes a headset with a semi-rigid boom and an O2 diffuser. The OA was compared to the Venturi mask in eight healthy adults after informed consent. Inspired O2 fractions were measured in the hypopharynx using continuous gas sampling at low to high O2 flow rates. Mean data were compared using two-tailed paired t tests with significance set at 0.05.
Results
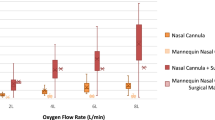
The measured inspired O2 concentration was higher in the OA at 2 (26.3 ± 2.5vs 23.3 ± 0.5,P < 0.01) and 6 L·min−1 (33.5 ± 3.3vs 28.8 ± 1.2,P < 0.01) flow rates. At 12 L·min−1, the O2 concentration was less in the OA (39.2 ± 6.3 vs 46.0 ± 2.7,P < 0.02). All subjects found both systems comfortable for the short duration of the study.
Conclusions
The OA delivered predictable concentrations of O2 over low to medium flow rates. This system is comfortable, easy to use, non-obtrusive, odorless, and latex-free. The ability to monitor capnography makes this device ideal for monitored anesthesia care or in other settings (intensive care) where monitoring of respiration is warranted. This device does not contact the face and thus may be ideal for pediatric patients and those on long-term home O2 therapy. Further clinical trials in these areas are warranted.
Résumé
Objectif
Décrire la mise au point et la performance d’un nouveau système de distribution d’oxygène à contact minimal pour la respiration buccale et nasale, doté de capacités capnographiques.
Méthode
Les défis du développement et de la conception du prototype de l’OxyArm ™ (OA) sont présentés. De conception innovatrice, il utilise un casque de monture semi-rigide et un diffuseur d’O2. L’OA a été comparé au masque Venturi chez huit adultes en bonne santé ayant consenti au test. Les fractions d’O2 inspiré ont été mesurées dans l’hypopharynx grâce à un échantillonnage gazeux continu d’O2 de bas débit à haut débit. Les données moyennes ont été comparées selon des tests t bilatéraux appariés comportant des niveaux signifi catifs à 0,05.
Résultats
La concentration d’O2 inspiré a été plus élevée avec l’OA pour des débits de 2 (26,3 ± 2,5 vs 23,3 ± 0,5,P < 0,01) et de 6 L·min−1 (33,5± 3,3 vs 28,8 ± 1,2, P < 0,01). Pour un débit de 12 L·min−1, la concentration d’O2 a été plus faible avec l’OA (39,2 ± 6, 3vs 46,0 ± 2,7, P < 0,02). Tous les sujets ont jugé les appareils confortables pendant l’étude de courte durée.
Conclusion
L’OA a distribué des concentrations prévisibles d’O2 de débits bas à moyens. Ce système est confortable, facile à utiliser, non obstructif, inodore et sans latex. Les possibilités capnographiques de cet appareil font qu’il est idéal pour l’anesthésie avec monitorage ou d’autres installations (soins intensifs) où le monitorage de la respiration est justifié. L’appareil n’entre pas en contact avec le visage, le rendant idéal pour la pédiatrie et l’oxygénothérapie de longue durée à domicile. Il faut d’ailleurs poursuivre les essais cliniques dans ce sens.
Article PDF
Similar content being viewed by others


References
Stewart BN, Hood CI, Block AJ. Long-term results of continuous oxygen therapy at sea level. Chest 1975; 68: 486–92.
Craig DB. Postoperative recovery of pulmonary function. Anesth Analg 1981; 60: 46–52.
Miller WF. Oxygen therapy, catheter, mask, hood and tent. Anesthesiology 1962; 23: 445–51.
Nolan KM, Baxter MK, Winyard JA, Roulson CJ, Goldhill DR. Video surveillance of oxygen administration by mask in postoperative patients. Br J Anaesth 1992; 69: 194–6.
Hoffman LA, Dauber JH, Ferson PF, Openbrier DR, Zullo TG. Patient response to transtracheal oxygen delivery. Am Rev Respir Dis 1987; 135: 153–6.
Merino-Angulo J, Perez de Diego I, Casas JM. Subcutaneous emphysema as a complication of oxygen therapy using nasal cannulas (Letter). N Engl J Med 1987; 316: 756.
Camner P, Bakke B. Nose or mouth breathing? Environ Res 1980; 21: 394–8.
Canet J, Sanchis J. Performance of a low flow O2 Venturi mask: diluting effects of the breathing pattern. Eur J Respir Dis 1984; 65: 68–73.
Kauffmann F, Annesi I, Neukirch F, Oryszczyn MP, Alpérovitch A. The relation between snoring and smoking, body mass index, age, alcohol consumption and respiratory symptoms. Euro Respir J 1989; 2: 599–603.
Nolan KM, Winyard JA, Goldhill DR. Comparison of nasal cannulae with face mask for oxygen administration to postoperative patients. Br J Anaesth 1993; 70: 440–2.
Kumar RM, Kabra SK, Singh M. Efficacy and acceptability of different modes of oxygen administration in children: implications for a community hospital. J Trop Pediatr 1997; 43: 47–9.
Author information
Authors and Affiliations
Corresponding author
Additional information
Developmental work was carried out at Southmedic Inc., and clinical work at Dr. S. McDonald’s office in Barrie, Ontario. Supported by a grant from Southmedic, Inc. of Barrie, Ontario, Canada.
Rights and permissions
About this article
Cite this article
Ling, E., McDonald, L., Dinesen, T.R.J. et al. The OxyArm™ — a new minimal contact oxygen delivery system for mouth or nose breathing. Can J Anesth 49, 297–301 (2002). https://doi.org/10.1007/BF03020531
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03020531