
Abstract
Purpose
To evaluate the performance of two different continuous cardiac output monitoring systems based on the thermodilution principle in critically ill patients.
Methods
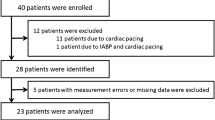
Nineteen cardiac surgical patients were randomly assigned to continuous cardiac output monitoring using one of the two systems under study (group I, IntelliCath™ catheter, n=9; group II, Opti-Q™ catheter,n = 10). Each patient was studied over a period of three hours. Conventional bolus thermodilution cardiac output measurements were carried out every 15 min leading to 13 measurements in each patient. The continuous cardiac output values were compared with the bolus thermodilution measurements. Bias (mean difference between continuous and bolus thermodilution) and precision (SD of differences) were calculated as a measure of agreement between the respective continuous method and conventional bolus thermodilution.
Results
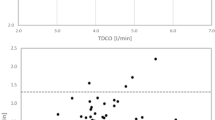
The range of measured cardiac outputs was 3.8–15.4 L·min−1 (IntelliCath™) and 3.5–8.3 L·min−1 (OptiQ™). Bias and precision was 0.06 ± 0.76 L·min−1 (IntelliCath™) and −0.04 ± 0.74 L·min−1 (OptiQ™), respectively. There was no difference in bias between the two systems (P=0.38). ± 2 SD of the differences (i.e., 95% of the differences) did not fall within the predetermined limits of agreement of ± 0.5 L·min−1.
Conclusions
There was no difference between the two systems regarding the agreement with conventional bolus thermodilution as the standard. A discrepancy between bolus and continuous thermodilution cardiac output measurement techniques above the clinically acceptable limits suggest that they are not interchangeable.
Résumé
Objectif
Évaluer, chez des patients gravement malades, la performance de deux systèmes de monitorage continu du débit cardiaque fondés sur le principe de la thermodilution.
Méthode
Dixneuf patients de cardiochirurgie ont été répartis de façon aléatoire en deux groupes de monltorage continu du débit cardiaque: le groupe I, avec une sonde IntelliCath™, n = 9; le groupe II, avec une sonde Opti- Q™, n = 10). Chaque patient a été observé pendant trois heures. Les mesures traditionnelles du débit cardiaque par thermodilution d’un bolus ont été faites toutes les 15 min, pour un total de 13 mesures par patient. Les valeurs continues du débit cardiaque ont été comparées aux mesures par thermodilution d’un bolus. Le biais (différence moyenne entre la thermodilution continue et celle d’un bolus) et la précision (écart type des différences) ont été calculés comme mesure de concordance entre la méthode continue et la thermodilution traditionnelle d’un bolus.
Résultats
Les limites des débits cardiaques mesurés ont été de 3,8 – 15,4 L·min− 1 (IntelliCath™ et de 3,5 – 8,3 L·min− 1 (OptiQ™). Le biais et la précision ont été de 0,06 ± 0,76 L·min− 1 (IntelliCath™) et de − 0,04 ± 0,74 L·min− 1 (OptiQ™), respectivement. Le biais a été comparable entre les deux sondes (P = 0,38); et ± 2 écarts types des différences (95 % des différences) n’étaient pas compris dans les limites de concordance prédéterminées de ± 0,5 L·min− 1.
Conclusion
Les deux systèmes n’ont pas présenté de différence entre eux quant à la concordance avec la norme traditionnelle de la thermodilution d’un bolus. Une divergence entre les mesures du débit cardiaque par themodilution d’un bolus et thermodilution continue au delà des limites acceptables en pratique permet d’affirmer que ces deux techniques ne sont pas interchangeables.
Article PDF
Similar content being viewed by others

References
Ganz W, Donoso R, Marcus HS, Forrester JS, Swan HJC. A new technique for measurement of cardiac output by thermodilution in man. Am J Cardiol 1971; 27: 392–6.
Forrester JS, Ganz W, Diamond G, McHugh F, Chonette DW, Swan HJC. Thermodilution cardiac output determination with a single flow-directed catheter. Am Heart J 1972; 83: 306–11.
Telderman ML, Ramsay MA, Quinn MD, Paulsen AW, McKown RC, Gillmann HP. Continuous thermodilution cardiac output measurement in intensive care unit patients. J Cardiothorac Vasc Anesth 1992; 6: 270–4.
Burchell SA, Yu M, Fakiguchi SA, Ohta RM, Myers SA. Evaluation of a continuous cardiac output and mixed venous oxygen saturation catheter in critically ill surgical patients. Crit Care Med 1997; 25: 388–91.
Mihm FG, Gettinger A, Hanson W, et al. A multicenter evaluation of a new continuous cardiac output pulmonary artery catheter system. Crit Care Med 1998; 26: 1346–50.
Zöllner C, Polasek J, Kilger E, et al. Evaluation of a new continuous thermodilution cardiac output monitor in cardiac surgical patients: a prospective criterion standard study. Crit Care Med 1999; 27: 293–8.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 8: 307–10.
Hardy J-F, Bélisle S, Gravel N. Incorrect analysis of data leads to incorrect conclusions. Can J Anaesth 1997; 44: 786–7.
Schmid ER, Spahn DR, Tornic M. Reliability of a new generation transesophageal doppler device for cardiac output monitoring. Anesth Analg 1993; 77: 971–9.
Sageman WS, Amundson DE. Thoracic electrical bioim pedance measurement of cardiac output in postaortocoronary bypass patients. Crit Care Med 1993; 21: 1139–42.
Perrino AC, Lippman A, Ariyan C, O`Conner TZ, Luther M. Intraoperative cardiac output monitoring: Comparison of impedance cardiography and thermodilution. J Cardiothorac Vasc Anesth 1994; 8: 24–9.
Philip JH, Long MC, Quinn MD, Newbower RS. Continuous thermal measurement of cardiac output. IEEE Trans Biomed Eng 1984; 5: 393–400.
Normann RA, Johnson RW, Messinger JE, Sohrab B. A continuous cardiac output computer based on thermodilution principles. Ann Biomed Eng 1989; 17: 61–73.
Yelderman M. Continuous measurement of cardiac output with the use of stochastic system identification techniques. J Clin Monit 1990; 6: 322–32.
Hogue CW, Rosenbloom M, McCawley C, Lappas DG. Comparison of cardiac output measurement by continuous thermodilution with electromagnetometry in adult cardiac surgical patients. J Cardiothorac Vasc Anesth 1994; 8: 631–5.
Lichtenthal PR, Wade LD. Continuous cardiac output measurements. J Cardiothorac Vasc Anesth 1994; 8: 668–70.
Jakobsen C-J, Melsen NC, Andresen EB. Continuous cardiac output measurements based on thermodilution technique in the perioperative period. J Cardiothorac Vasc Anesth 1994; 8 Suppl 3: 47.
Böttiger BW, Soder M, Rauch H, et al. Semi-continuous versus injectate cardiac output measurement in intensive care patients after cardiac surgery. Intensive Care Med 1996; 22: 312–8.
Jacquet L, Hanique G, Glorieux D, Matte P, Goenen M. Analysis of the accuracy of continuous thermodilution cardiac output measurement. Intensive Care Med 1996; 22: 1125–9.
Boldt J, Menges T, Wollbrück M, Hammermann H, Hempelmann G. Is continuous cardiac output measurement using thermodilution reliable in the critically ill patient? Crit Care Med 1994; 22: 1913–8.
Hatter M, Zöllner C, Briegel J, Forst H. Evaluation of a new continuous thermodilution cardiac output monitor in critically ill patients: A prospective criterion standard study. Crit Care Med 1995; 23: 860–6.
Aranda M, Mihm FG, Garrett S, Mihm MN, Pearl RG. Continuous cardiac output catheters. Delay in in vitro response time after controlled flow changes. Anesthesiology 1998; 89: 1592–5.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zöllner, C., Goetz, A.E., Weis, M. et al. Continuous cardiac output measurements do not agree with conventional bolus thermodilution cardiac output determination. Can J Anesth 48, 1143–1147 (2001). https://doi.org/10.1007/BF03020382
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03020382