
Abstract
Purpose: To quantify the effects of graded head rotation and elevation on intracranial pressure (ICP) in neurosurgical patients, before and after induction of general anesthesia.
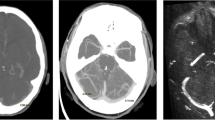
Methods: Patients with supratentorial tumours (n=12), scheduled for craniotomy with planned ICP monitoring, underwent baseline ICP measurements awake and supine (0° rotation and elevation). Incremental degrees of head rotation (15°) and of head elevation (10°) were performed independently and in combination. Paired measurements of ICP at all levels of head rotation and elevation were also performed before and after induction of general anesthesia (n=6).
Results: The baseline ICP was 12.3±6.4 mmHg (n=12). Changes of ICP were proportional to the degree of head rotation or elevation. Head rotation of 60° maximally increased ICP to 24.8±14.3 mmHg (P<0.05). Head elevation above 20° reduced ICP, with a maximal reduction to −0.2±5.5 mmHg at 40° elevation (P<0.01). Head elevation to 30° reduced the intracranial hypertension associated with head rotation. No differences were observed between ICP measurements made before or after induction of general anesthesia (n=6). Three patients experienced headache with extreme head rotation (<60°) and intracranial hypertension (ICP>20 mmHg).
Conclusion: Head rotation of 60° caused an increase in ICP. Concomitant head elevation to 30° reduced the intracranial hypertension associated with head rotation. Headache with head rotation may provide a useful clinical warning of elevated ICP.
Résumé
Objectif: Quantifier les effets de la rotation et de l’élévation graduées de la tête sur la tension intracrânienne (TIC) chez des patients de neurochirurgie, avant et après l’induction de l’anesthésie générale.
Méthode: Des patients atteints de tumeurs sus-tentorielles (n=12) devaient subir une craniotomie sous monitorage planifié de la TIC. On a mesuré les valeurs de base de la TIC à l’état d’éveil et en position couchée sur le dos (0° de rotation et d’élévation). Des changements incrémentiels du degré de rotation (15°) et d’élévation de la tête (10°) ont été réalisés, indépendants les uns des autres et combinés. Les mesures appariées de TIC pour tous les degrés de rotation et d’élévation de la tête ont aussi été faites avant et après l’induction de l’anesthésie générale (n=6).
Résultats: La TIC de base était de 12,3±6,4 mmHg (n=12). Les changements de TIC on été proportionnels au degré de rotation et d’élévation d la tête. La rotation de 60° a conduit à la TIC maximale de 24,8±14,3 mmHg (P<0,05). L’élévation au-dessus de 20° a réduit la TIC, la réduction maximale étant de −0,2±5,5 mmHg à 40° d’élévation (P<0,01). L’élévation de la tête à 30° a réduit l’hypertension intracrânienne associée à la rotation de la tête. Aucune différence de TIC n’a été notée entre les mesures prises avant ou après l’induction de l’anesthésie générale (n=6). Trois patients ont éprouvé des céphalées au moment de la rotation extrême de la tête (<60°) et une hypertension intracrânienne (TIC)>20 mmHg.
Conclusion: La rotation de la tête de 60° a causé une augmentation de la TIC. L’élévation concomitante de la tête à 30° a réduit la TIC associée à la rotation de la tête. Les céphalées associées à la rotation de la tête peuvent servir d’indice clinique d’une TIC élevée.
Article PDF
Similar content being viewed by others

References
Lyons MK, Meyer FB. Cerebrospinal fluid physiology and the management of increased intracranial pressure. Mayo Clin Proc 1990; 65: 684–707.
Frank JI. Management of intracranial hypertension. Med Clin North Am 1993; 77: 61–76.
Simmons BJ. Management of intracranial hemodynamics in the adult: a research analysis of head positioning and recommendations for clinical practice and future research. J Neursci Nurs 1997; 29: 44–9.
Durward QJ, Amacher AL, Del Maestro RF, Sibbald WJ. Cerebral and cardiovascular responses to changes in head elevation in patients with intracranial hypertension. J Neurosurg 1983; 59: 938–44.
Emery JR, Peabody JL. Head position affects intracranial pressure in newborn infants. J Pediatr 1983; 103: 950–3.
Rosner MJ, Coley IB. Cerebral perfusion pressure, intracranial pressure, and head elevation. J Neurosurg 1986; 65: 636–41.
Feldman Z, Kanter MJ, Robertson CS, et al. Effect of head elevation on intracranial pressure, cerebral perfusion pressure, and cerebral blood flow in head-injured patients. J Neurosurg 1992; 76: 207–11.
Schneider G-H, v Helden A, Franke R, Lanksch WR, Unterberg A. Influence of body position on jugular venous oxygen saturation, intracranial pressure and cerebral perfusion pressure. Acta Neurochir 1993; 59(Suppl): 107–12.
Meixensberger J, Baunach S, Amschler J, Dings J, Roosen K. Influence of body position on tissue-pO2, cerebral perfusion pressure and intracranial pressure in patients with acute brain injury. Neurol Res 1997; 19: 249–53.
Lipe HP, Mitchell PH. Positioning the patient with intracranial hypertension: how turning and head rotation affect the internal jugular vein. Heart Lung 1980; 9: 1031–7.
Williams A, Coyne SM. Effects of neck position on intracranial pressure. Am J Crit Care 1993; 2: 68–71.
Goldberg RN, Joshi A, Moscoso P, Castillo T. The effect of head position on intracranial pressure in the neonate. Crit Care Med 1983; 11: 428–30.
Chambers IR, Kane PJ, Choksey MS, Mendelow AD. An evaluation of the Camino ventricular bolt system in clinical practice. Neurosurgery 1993; 33: 866–8.
Craig GR, Nielsen MS. Rigid cervical collars and intracranial pressure. Intensive Care Med 1991; 17: 504–5.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was funded in part by a grant from Janssen Pharmaceutica Canada, Toronto, Ontario.
Rights and permissions
About this article
Cite this article
Hung, O.R., Hare, G.M.T. & Brien, S. Head elevation reduces head-rotation associated increased ICP in patients with intracranial tumours. Can J Anaesth 47, 415–420 (2000). https://doi.org/10.1007/BF03018970
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018970