
Abstract
Purpose
Dental damage may occur with laryngoscopy. The purpose of this study was twofold : to determine whether preoperative examination could predict the risk of contacting the teeth with the laryngoscope and to evaluate the effectiveness of a modified Macintosh blade on reducing dental contact.
Methods
Four hundred and eighty-three patients scheduled for elective surgery requiring general anesthesia with endotracheal tube placement were studied prospectively. Features that might predict difficult intubation were assessed preoperatively. Laryngoscopy was performed twice on each patient, once with a regular Macintosh 3 blade and once with a blade in which the flange was partially removed (Callander modification). The distance between the flange of the blade and the upper incisors at glottic exposure was measured. We calculated correlations between individual airway characteristics and the chance of hitting the upper teeth with the regular Macintosh 3 blade and compared the frequencies of contacting the teeth between the two blades.
Results
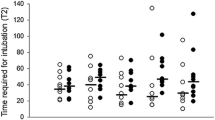
The chance of hitting the upper teeth when using the regular Macintosh 3 blade increased significantly with non-parametric scores for Mallampati classification, mandibular subluxation, head and neck movement, interincisor gap, and condition of the upper teeth. (P < 0.01) The frequency of direct contact varied significantly between the two blades: 20.3% vs 4.1% for Macintosh 3 and modified blades, respectively (P < 0.05). Laryngeal views were improved with the modified blade.
Conclusion
Airway characteristics correlate with the risk of hitting the upper teeth during laryngoscopy. The modified Macintosh blade reduces the risk of contacting the teeth.
Résumé
Objectif
La laryngoscopie peut provoquer des lésions aux dents. Notre double objectif était : de déterminer si l’examen préopératoire peut permettre de prédire le risque de toucher les dents avec le laryngoscope et d’évaluer l’efficacité d’une lame Macintosh modifiée sur la réduction de contact avec les dents.
Méthode
Des patients (483) devant subir une intervention chirurgicale réglée nécessitant une anesthésie générale avec la mise en place d’un tube endotrachéal ont participé à notre étude prospective. Nous avons fait l’évaluation préopératoire des caractéristiques permettant de prédire une intubation difficile. La laryngoscopie a été réalisée deux fois sur chaque patient, avec une lame Macintosh 3 ordinaire et avec une lame dont le connecteur à bride avait été partiellement enlevé (modification Callander). La distance entre le manche de la lame et les incisives supérieures a été mesurée à l’exposition de la glotte. Nous avons calculé les corrélations entre les caractéristiques individuelles des voies aériennes et le risque de toucher les dents supérieures avec la lame Macintosh 3 ordinaire, et comparé les fréquences de contact avec les dents pour les deux lames.
Résultats
Le risque de toucher les dents supérieures avec la lame Macintosh 3 ordinaire augmente significativement avec les scores non-paramétriques de la classification de Mallampati, la subluxation mandibulaire, le mouvement de la tête et du cou, l’espace inter-incisive et l’état de la dentition supérieure (P < 0,01). La fréquence de contact direct varie significativement d’une lame à l’autre : 20,3 % vs 41% respectivement pour la lame Macintosh 3 et la lame modifiée (P < 0,05). Les visualisations du larynx sont meilleures avec la lame modifiée.
Conclusion
Il existe une corrélation entre les caractéristiques des voies aériennes et le risque de toucher les dents supérieures pendant la laryngoscopie. La lame Macintosh modifiée réduit ce risque.
Article PDF
Similar content being viewed by others


References
Owen H, Waddell-Smith I. Dental trauma associated with anaesthesia. Anaesth Intensive Care 2000; 28: 133–45.
Warner ME, Benenfeld SM, Warner MA, Schroeder DR, Maxson PM. Perianesthetic dental injuries. Frequency, outcomes, and risk factors. Anesthesiology 1999; 90: 1302–5.
Callander CC, Thomas J. Modification of Macintosh laryngoscope for difficult intubation (Letter). Anaesthesia 1987; 42: 671–2.
Benumof JL. Management of the difficult adult airway. With special emphasis on awake tracheal intubation. Anesthesiology 1991; 75: 1087–110.
Wilson ME, Spiegelhalter D, Robertson JA, Lesser P. Predicting difficult intubation. Br J Anaesth 1988; 61: 211–6.
Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia 1984; 39: 1105–11.
Benumof JL. The unanticipated difficult airway (Letter). Can J Anesth 1999; 46: 510–1.
Watanabe S, Suga A, Asakura N, et al. Determination of the distance between the laryngoscope blade and the upper incisors during direct laryngoscopy: comparisons of a curved, an angulated straight, and two straight blades. Anesth Analg 1994; 79: 638–41.
Bito H, Nishiyama T, Higarhizawa T, Sakai T, Konishi A. Determination of the distance between the upper incisors and the laryngoscope blade during laryngoscopy: comparisons of the McCoy, the Macintosh, the Miller, and the Belscope blades (Japanese). Masui 1998; 47: 1257–61.
Bucx MJ, Snijders CJ, van der Vegt MH, Holstein JD, Stijnen T. Reshaping the Macintosh blade using biomechanical modelling. A prospective comparative study in patients. Anaesthesia 1997; 52: 662–7.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors wish to acknowledge the financial support of the Catholic Medical Center Research Foundation made in the program year of 2003.
Rights and permissions
About this article
Cite this article
Lee, J., Choi, J.H., Lee, Y.K. et al. The callander laryngoscope blade modification is associated with a decreased risk of dental contact. Can J Anesth 51, 181–184 (2004). https://doi.org/10.1007/BF03018781
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018781