
Abstract
Purpose
To date, no monitoring has proved its usefulness for both interpretation and treatment of arterial hypotension following pheochromocytoma resection. In this prospective observational study we measured the negative component (Δdown) of the respiratory systolic pressure variation in order to assess its ability to guide fluid therapy in 13 patients undergoing pheochromocytoma surgery.
Methods
The arterial pressure waveform was recorded via a 20-g radial artery catheter. Δdown was measured during abdominal exploration (baseline), after fluid loading, before and following tumour resection, and during treatment of arterial hypotension.
Results
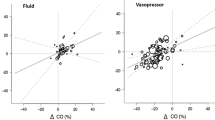
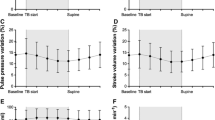
At baseline, Δdown ranged between I and 15 mmHg (median: 3 mmHg). Volume loading (500 mL colloid over 20 min) performed during abdominal exploration significantly reduced Adown (P = 0.001) and resulted in Adown values ≤ 2 mmHg in all 13 patients. The Δdown measured immediately before resection was larger in patients who had arterial hypotension (systolic arterial pressure (SAP) < 90 mmHg) following tumour removal than in other patients [4 (1–10)vs 1 (0–3) mmHg;P = 0.04], During hypotension, Δdown was greater in patients where fluid replacement restored SAP than in patients where fluids were ineffective and vasopressors needed [Δdown: 4 (3–9)vs 1 (1–2) mmHg;P = 0.03].
Conclusion
During pheochromocytoma surgery, a Δdown ≤ 2 mmHg appears to indicate minimal intravascular volume depletion. Δdown measurements could be used to guide fluid therapy for the prevention and treatment of arterial hypotension following pheochromocytoma removal.
Résumé
Objectif
Aucun monitorage n’est encore utile à l’interprétation et au traitement de l’hypotension artérielle qui suit la résection d’un phéochromocytome. Pendant notre étude prospective par observa-tion, nous avons mesuré la composante négative (Δdown) de la variation de la pression systolique respiratoire afin d’évaluer sa capacité à guider le remplissage vasculaire chez 13 patients opérés pour un phéochromocytome.
Méthode
La pression artérielle a été enregistrée au moyen d’un cathéter artériel radial de calibre 20. Le Δdown a été mesuré pendant l’exploration abdominale (mesure de base), après la charge liquidienne, avant et après la résection tumorale et pendant le traitement de l’hypotension artérielle.
Résultats
Au départ, le Δdown se situait entre 1 et 15 mmHg (médiane : 3 mmHg). La charge volumique (500 mL de colloïde pendant 20 min) réalisée pendant l’exploration abdominale a significativement réduit le Δdown (P = 0,001) et entraîné des valeurs ≤ 2 mmHg chez les 13 patients. Le Δdown mesuré immédiatement avant la résection a été plus important chez les patients qui avaient de l’hypotension artérielle (pression artérielle systolique (PAS) < 90 mmHg) après le retrait de la tumeur que chez les autres patients [4 (1–10) vs 1 (0–3) mmHg; P = 0,04]. Pendant l’hypotension, le Δdown était plus marqué pour les patients chez qui le remplacement liquidien a restauré la PAS que pour les patients où les liquides ont été inefficaces et les vaso-presseurs nécessaires [Δdown : 4 (3–9) vs 1 (1–2) mmHg; P = 0,03].
Conclusion
Pendant la résection d’un phéochromocytome, un Δdown ≤ 2 mmHg semble indiquer une déplétion minimale du volume des liquides intravasculaires. Les mesures du Δdown peuvent guider le remplissage vasculaire utilisé comme prévention et traitement de l’hypotension artérielle suivant la résection d’un phéochromocytome.
Article PDF
Similar content being viewed by others
References
Desmonts JM, Le Houelleur J, Remond P, Duvaldestin P. Anaesthetic management of patients with phaeochromocytoma. A review of 102 cases. Br J Anaesth 1977; 49: 991–8.
Rotzen MF. Anesthetic implications of concurrent diseases.In: Miller RD (Ed.). Anesthesia. New York: Churchill Livingstone Inc.; 1994: 903–1014.
Mihm FG. Pulmonary artery pressure monitoring in patients with pheochromocytoma. Anesth Analg 1983; 62: 1129–33.
Pinaud M, Desjars P, Tasseau F, Cozian A. Preoperative acute volume loading in patients with pheochromocytoma. Crit Care Med 1985; 13: 460–3.
Hull CJ. Phaeochromocytoma. Diagnosis, preoperative preparation and anaesthetic management. Br J Anaesth 1986; 58: 1453–68.
Michard F, Teboul JL. Using heart-lung interactions to assess fluid responsiveness during mechanical ventilation. Crit Care 2000; 4: 282–9.
Perel A, Pizov R, Cotev S. Systolic blood pressure variation is a sensitive indicator of hypovolemia in ventilated dogs subjected to graded hemorrhage. Anesthesiology 1987; 67: 498–502.
Coriat P, Vrillon M, Perel A, et al. A comparison of systolic blood pressure variations and echocardiographic estimates of end-diastolic left ventricular size in patients after aortic surgery. Anesth Analg 1994; 78: 46–53.
Rooke GA, Schwid HA, Shapiro, Y. The effect of graded hemorrhage and intravascular volume replacement on systolic pressure variation in humans during mechanical and spontaneous ventilation. Anesth Analg 1995; 80: 925–32.
Tavernier B, Makhotine O, Lebuffe G, Dupont J, Scherpereel P. Systolic pressure variation as a guide to fluid therapy in patients with sepsis-induced hypotension. Anesthesiology 1998; 89: 1313–21.
Michard F, Boussat S, Chemla D, et al. Relation between respiratory changes in arterial pulse pressure and fluid responsiveness in septic patients with acute circulatory failure. Am J Respir Crit Care Med 2000; 162: 134–8.
Proye C, Thevenin D, Cecat P, et al. Exclusive use of calcium channel blockers in preoperative and intraoperative control of pheochromocytomas: hemodynamics and free catecholamine assays in ten consecutive patients. Surgery 1989; 106: 1149–54.
Bravo EL, Gifford RW Jr. Pheochromocytoma: diagnosis, localization and management. N Engl J Med 1984; 311: 1298–303.
Pinsky MR. Functional hemodynamic monitoring. Intensive Care Med 2002; 28: 386–8.
Shupak RC. Difficult anesthetic management during pheochromocytoma surgery. J Clin Anesth 1999; 11: 247–50.
Kinney MA, Warner ME, van Heerden JA, et al. Perianesthetic risks and outcomes of pheochromocytoma and paraganglioma resection. Anesth Analg 2000; 91: 1118–23.
Prys-Roberts C. Phaeochromocytoma-recent progress in its management. Br J Anaesth 2000; 85: 44–57.
Stoneham MD. Less is more…using systolic pressure variation to assess hypovolaemia (Editorial). Br J Anaesth 1999; 83: 550–1.
Tavernier B. Evaluation peropératoire de la volémie.In: Société Française d’Anesthésie et de Réanimation (Ed.). Conférences d’Actualisation, Paris: Editions scientifiques et médicales Elsevier SAS et SFAR; 2001: 385–98.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mallat, J., Pironkov, A., Destandau, MS. et al. Systolic pressure variation (Δdown) can guide fluid therapy during pheochromocytoma surgery. Can J Anesth 50, 998–1003 (2003). https://doi.org/10.1007/BF03018362
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018362