
Abstract
Purpose
The low incidence of mortality and major morbidity in anesthesia makes it difficult to study the pattern of potential accidents and to develop preventive strategies. Anesthetic ‘near-misses’, however, occur more frequently. Using data from a simple routine-based system of problem reporting, we have analyzed the pattern and causes of serious non-fatal problems, in order to improve preventive strategies.
Methods
We prospectively recorded anesthesia-related information from all anesthetics for five years. The data included intraoperative problems, which were graded into four levels, according to severity. We analyzed only the serious nonfatal problems, which were sorted according to clinical presentation, and also according to which factor was most important in the development of the problem. We assessed any untoward consequences for the patient, and whether the problems could have been prevented.
Results
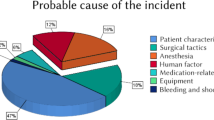
Serious problems were recorded in 315 cases out of 83,844 (0.4%). Anesthesia was considered the major contributing factor in III cases. Difficult intubation, difficult emergence from general anesthesia, allergic reactions, arrhythmia and hypotension were the dominating problems. Twenty-six anesthesia related problems resulted in changes in level of postoperative care, and one patient later died in the intensive care unit after anaphylactic shock. Eighty-two problems could have been prevented by simple strategies.
Conclusion
Analysis of serious nonfatal problems during anesthesia may contribute to improved preventive strategies. Data from a routine-based system are suitable for this type of analysis. Intubation, emergence, arrhythmia, hypotension and anaphylaxis cause most serious problems, and should be the object of preventive strategies.
Résumé
Objectif
La faible incidence de mortalité et de morbidité importante en anesthésie complique l’étude des types d’accidents potentiels et la mise au point de stratégies préventives. Les quasi accidents anesthésiques, par contre, surviennent plus fréquemment. En utilisant les données d’un simple système de notification de cours normal, nous avons analysé le type et les causes de problèmes graves, non mortels, dans le but d’améliorer les stratégies préventives.
Méthode
Nous avons enregistré prospectivement les informations reliées à toutes les anesthésies réalisées pendant cinq ans. Les données comprenaient les problèmes peropératoires que nous avons classés selon quatre niveaux de sévérité. Nous avons analysé les problèmes graves, non mortels, qui ont été retenus d’après la présentation clinique et aussi en fonction du facteur le plus important de l’évolution du problème. Nous avons évalué toutes les conséquences négatives pour le patient et la possibilité de prévention de ces problèmes.
Résultats
Des problèmes graves ont été notés dans 315 cas sur 83 844 (0,4 %). Lanesthésie a été considérée comme le principal facteur dans III cas. L’intubation difficile, le retour à la conscience difficile après l’anesthésie générale, les réactions allergiques, l’arythmie et l’hypotension ont dominé le tableau. Vingt-six problèmes reliés à l’anesthésie ont entraîné la modification des soins postopératoires et un patient est décédé à l’unité des soins intensifs d’un choc anaphylactique. Quatre-vingt-deux problèmes auraient pu être évités par de simples interventions.
Conclusion
Lanalyse de problèmes graves, mais non mortels, survenus pendant l’anesthésie peut contribuer à l’amélioration de stratégies préventives. Les données obtenus d’un système régulier de notification sont pertinentes à ce genre d’analyse. L’intubation, le retour à la conscience, l’arythmie, l’hypotension et l’anaphylaxie causent les problèmes les plus graves et devraient être prévenus.
Article PDF
Similar content being viewed by others


References
Barach P, Small SD. Reporting and preventing medical mishaps: lessons from non-medical near miss reporting systems. BMJ 2000; 320: 759–63.
Billings CE. Some hopes and concerns regarding medical event-reporting systems. Lessons from the NASA Aviation Safety Reporting System (Editorial). Arch Pathol Lab Med 1998; 122: 214–5.
Helmreich RL. On error management: lessons from aviation. BMJ 2000; 320: 781–5.
Gaba DM, Maxwell M, DeAnda A. Anesthetic mishaps: breaking the chain of accident evolution. Anesthesiology 1987; 66: 670–6.
Cooper JB. How to measure what happens. Can J Anaesth 1991; 38: 1032–3.
Cohen MM, Duncan PG, Pope WDB, et al. The Canadian four-centre study of anaesthetic outcomes: II. Can outcomes be used to assess the quality of anaesthesia care? Can J Anaesth 1992; 39: 430–9.
Lee A, Lum ME. Measuring anaesthetic outcomes. Anaesth Intensive Care 1996; 24: 685–93.
Fasting S, Gisvold SE. Data recording of problems during anaesthesia: presentation of a well-functioning and simple system. Acta Anaesthesiol Scand 1996; 40: 1173–83.
Vleeming W, van Amsterdam JGC, Stricker BHC, de Wildt DJ. ACE inhibitor-induced angioedema. Incidence, prevention and management. Drug Saf 1998; 18: 171–88.
Cooper JB, Cullen DJ, Nemeskal R, et al. Effects of information feedback and pulse oximetry on the incidence of anesthesia complications. Anesthesiology 1987; 67: 686–94.
Spencer FC. Human error in hospitals and industrial accidents: current concepts. J Am Coll Surg 2000; 191: 410–8.
Orkin FK, Cohen MM, Duncan PG. The quest for meaningful outcomes. Anesthesiology 1993; 78: 417–22.
Sanborn KV, Castro J, Kuroda M, Thys DM. Detection of intraoperative incidents by electronic scanning of computerized anesthesia records. Comparison with voluntary reporting. Anesthesiology 1996; 85: 977–87.
Cooper JB. Is voluntary reporting of critical events effective for quality assurance? Anesthesiology 1996; 85: 961–4.
Cullen DJ Bates DW, Small SD, Cooper JB, Nemeskal AR, Leape LL. The incident reporting system does not detect adverse drug events: a problem for quality improvement. Jt Comm J Qual Improv 1995; 21: 541–8.
Jayasuriya JP, Anandaciva S. Compliance with an incident report scheme in anaesthesia. Anaesthesia 1995; 50: 846–9.
Cohen MR. Why error reporting systems should be voluntary. BMJ 2000; 320: 728–9.
Schwilk B, Muche R, Bothner U, Goertz A, Friesdorf W, Georgieff M. Quality control in anesthesiology. Results of a prospective study following the recommendations of the German Society of Anesthesiology and Intensive Care (German). Anaesthesist 1995; 44: 242–9.
Schwilk B, Muche R, Treiber H, Brinkmann A, Georgieff M, Bothner U. A cross-validated multifactorial index of perioperative risks in adults undergoing anaesthesia for non-cardiac surgery. Analysis of perioperative events in 26907 anaesthetic procedures. J Clin Monk Comput 1998; 14: 283–94.
Bothner U, Georgieff M, Schwilk B. Building a large-scale perioperative anaesthesia outcome-tracking data-base: methodology, implementation, and experiences from one provider within the German quality project. Br J Anaesth 2000; 85: 271–80.
Sigurdsson GH, McAteer E. Morbidity and mortality associated with anaesthesia. Acta Anaesthesiol Scand 1996; 40: 1057–63.
Stienstra R. Mechanisms behind and treatment of sudden, unexpected circulatory collapse during central neuraxis blockade. Acta Anaesthesiol Scand 2000; 44: 965–71.
Runciman WB. Risk assessment in the formulation of anaesthesia safety standards. Eur J Anaesthesiol Suppl 1993; 10(Suppl. 7): 26–32.
Tiret L, Desmonts JM, Hatton F, Vourc’h G. Complications associated with anaesthesia—a prospective survey in France. Can Anaesth Soc J 1986; 33: 336–44.
Caplan RA, Posner KL, Ward RJ, Cheney FW. Adverse respiratory events in anesthesia: a closed claims analysis. Anesthesiology 1990; 72: 828–33.
Rose DK, Cohen MM. The airway: problems and predictions in 18,500 patients. Can J Anaesth 1994; 41: 372–83.
Rose DK, Cohen MM. The incidence of air-way problems depends on the definition used. Can J Anaesth 1996; 43: 30–4.
Randell T. Prediction of difficult intubation. Acta Anaesthesiol Scand 1996; 40: 1016–23.
El-Ganzouri AR, McCarthy RJ, Tuman KJ, Tanck EN, Ivankovich AD. Preoperative airway assessment: predictive value of a multivariate risk index. Anesth Analg 1996; 82: 1197–204.
Arné J, Descoins P, Fusciardi J, et al. Preoperative assessment for difficult intubation in general and ENT surgery: predictive value of a clinical multivariate risk index. Br J Anaesth 1998; 80: 140–6.
Crosby ET, Cooper RM, Douglas MJ, et al. The unanticipated difficult airway with recommendations for management. Can J Anaesth 1998; 45: 757–76.
Løvstad RZ, Granhus G, Hetland S. Bradycardia and asystolic cardiac arrest during spinal anaesthesia: a report of five cases. Acta Anaesthesiol Scand 2000; 44: 48–52.
Laxenaire MC et le Groupe d’etudes des réactions anaphylactoïdes peranesthésiques. Épidémiologie des réactions anaphylactoïdes peranesthésiques. Quatrième enquête multicentrique (juillet 1994-décembre 1996). Ann Fr Anesth Reanim 1999; 18: 796–809.
Laxenaire MC, Mertes PM, and Groupe d’Etudes des Réactions Anaphylactoïdes Peranesthésiques. Anaphylaxis during anaesthesia. Results of a two-year survey in France. Br J Anaesth 2001; 87: 549–58.
Fasting S, Søreide E, Raeder JC. Changing preoperative fasting policies. Impact of a national consensus. Acta Anaesthesiol Scand 1998; 42: 1188–91.
Meilin Olsen J, Fasting S, Gisvold SE. Routine preoperative gastric emptying is seldom indicated. A study of 85 594 anaesthetics with special focus on aspiration pneumonia. Acta Anaesthesiol Scand 1996; 40: 1184–8.
Cohen MM, Duncan PG, Pope WDB, Wolkenstein C A survey of 112,000 anaesthetics at one teaching hospital (1975–83). Can Anaesth Soc J 1986; 33: 22–31.
Webb RK, Currie M, Morgan CA, et al. The Australian Incident Monitoring Study: an analysis of 2000 incident reports. Anaesth Intensive Care 1993; 21: 520–8.
Author information
Authors and Affiliations
Corresponding author
Additional information
The study is supported with grants from the Norwegian Medical Research Council.
Rights and permissions
About this article
Cite this article
Fasting, S., Gisvold, S.E. Serious intraoperative problems — a five-year review of 83,844 anesthetics. Can J Anesth 49, 545–553 (2002). https://doi.org/10.1007/BF03017379
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03017379