
Abstract
Purpose
To evaluate the combination of rectal indomethacin with patient controlled intravenous morphine analgesia (PCA) on postoperative pain relief and opioid use after cardiac surgery.
Methods
With institutional ethics approval, 57 consenting adults undergoing elective aortocoronary bypass surgery were randomly assigned preoperatively in a double-blind fashion to receive either placebo (n = 26) or indomethadn 100 mg suppositories (n = 31), 2–3 hr postoperatively, and 12 hr later. Both groups utilized PCA morphine. Pain scores in the two treatment groups were assessed on a 10-cm visual analogue scale (VAS) (at rest and with cough) at 4, 6, 12, 18 and 24 hr after initial dosing, and were analyzed through a 2 × 5 repeated measures of variance. The 24 hr analgesic consumption, 12 and 24 hr chest tube blood loss, and time to tracheal extubation were also recorded, and compared for the two treatment arms through Student’s t test on independent samples.
Results
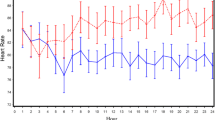
Postoperative morphine consumption in the first 24 hr was 38% less in the indomethadn group (22.40 ± 12.55 mg) than the placebo group (35.99 ± 25.84 mg), P= 0.019. Pain scores, measured with a VAS, were 26% to 66% lower in the indomethacinvs placebo group at rest (P=0.006), but not with cough, for all times assessed. There was no difference in blood loss (at 12 hr) or time to tracheal extubation for both groups.
Conclusion
The combination of indomethacin with morphine after cardiac surgery results in reduced postoperative pain scores and opioid use without an increase in side effects.
Résumé
Objectif
Évaluer l’action combinée d’indométhacine rectale et d’analgésie contrôlée par le patient (ACP) avec de la morphine intraveineuse sur la douleur postopératoire et l’usage d’opioïde en cardiochirurgie.
Méthode
Ayant obtenu l’approbation du comité d’éthique de l’hôpital, 57 adultes consentants qui devaient subir un pontage aortocoronarien électif ont été répartis au hasard avant l’opération afin de recevoir en double insu, soit un placebo (n = 26), soit de l’indométhacine (n = 31) en suppositoires de 100 mg, 2–3 h après l’opération et 12 h plus tard. Tous ont utilisé de la morphine pour l’ACP. Les scores de douleur ont été évalués à l’aide d’une échelle visuelle analogue (EVA) de 10 cm (au repos et lors de la toux) à 4, 6, 12, 18 et 24 h après le dosage initial et analysés selon un plan 2 × 5 de mesures répétées de la variance. La consommation d’analgésique à 24 h, la perte sanguine au drain thoracique à 12 et 24 h et le moment de l’extubation endotrachéale ont été notés et comparés d’un groupe à l’autre par le test t de Student sur des échantillons indépendants.
Résultats
La demande postopératoire de morphine des 24 premières h a été de 38% moindre avec l’indométhacine (22,40 ± 12,55 mg) qu’avec le placebo (35,99 ± 25,84 mg),P = 0,019. Les scores de douleur de l’EVA ont été de 26% à 66% plus faibles pour l’indométhacine vs le placebo, au repos (P = 0,006), non lors de la toux, et ce, pour tous les temps de mesures. La perte sanguine a été semblable dans les deux groupes (à 12 h) ainsi que le temps total d’intubation.
Conclusion
Administrée après une intervention cardiaque, la combinaison d’indométhacine et de morphine a réduit les douleurs et l’usage d’opioïdes sans augmenter les effets secondaires.
Article PDF
Similar content being viewed by others


References
Maxam-Moore VA, Wilkie DJ, Woods SL. Analgesics for cardiac surgery patients in critical care: describing current practice. Am J Crit Care 1994; 3: 31–9.
Moote C. Efficacy of nonsteroidal anti-inflammatory drugs in the management of postoperative pain. Drugs 1992; 44(Suppl): 14–30.
Dahl JB, Kehlet H. Non-steroidal anti-inflammatory drugs: rationale for use in severe postoperative pain. Br J Anaesth 1991; 66: 703–12.
Nuutinen LS, Laitinen JO, Salomäki TE. A risk-benefit appraisal of injectable nsaids in the management of postoperative pain. Drug Safety 1993; 9: 380–93.
Souter AJ, Fredman B, White PF. Controversies in the perioperative use of nonsteroidal antiinflammatory drugs. Anesth Analg 1994; 79: 1178–90.
Reuben SS, Connelly NR, Lurte S, Klatt M, Gibson CS. Dose-response of ketorolac as an adjunct to patientcontrolled analgesia morphine after spinal surgery. Anesth Analg 1998; 87: 98–102.
Laitinen J, Nuutinen L. Intravenous diclofenac coupled with PCA fentanyl for pain relief after total hip replacement. Anesthesiology 1992; 76: 194–8.
Nissen I, Jensen KA, Öhrström JK. Indomethacin in the management of postoperative pain. Br J Anaesth 1992; 69: 304–6.
Pavy T, Medley C, Murphy DF, Effect of indomethacin on pain relief after thoracotomy. Br J Anaesth 1990; 65: 624–7.
Engel C, Lund B, Kristensen SS, Axel C, Nielsen JB. Indomethacin as an analgesic after hysterectomy. Acta Anaesth Scand 1989; 33: 498–501.
Keenan DJM, Cave K, Langdon L, Lea RE. Comparative trial of rectal indomethacin and cryoanalgesia for control of early postthoracotomy pain. BMJ 1983; 287: 1335–7.
Reasbeck PG, Rice ML, Reasbeck JC. Double-blind controlled trial of indomethacin as an adjunct to narcotic analgesia after major abdominal surgery. Lancet 1982; 2: 115–8.
Alván G, Orme M, Bertilsson L, Ekstrand R, Palmér L. Pharmacokinetics of indomethacin. Clin Pharmacol Ther 1975; 18: 364–73.
Cohen J. F tests on means in the analysis of variance and covariance.In: Statistical Power Analysis for the Behavioral Sciences, Revised ed. New Jersey: Academic Press, 1977: 273–406.
Sims C, Johnson CM, Bergesio R, Delfos SJ, Avraamides EA. Rectal indomethacin for analgesia after appendectomy in children. Anaesth Intensive Care 1994; 22: 272–5.
Turner GA, Gorringe J. Indomethacin as adjunct analgesia following open cholecystectomy. Anaesth Intensive Care 1994; 22: 25–9.
Parker RK, Holtmann B, Smith I, White PF. Use of ketorolac after lower abdominal surgery. Effect on analgesic requirement and surgical outcome. Anesthesiology 1994; 80: 6–12.
Eriksson H, Tenhunen T, Korttila K. Balanced analgesia improves recovery and outcome after outpatient tubal ligation. Acta Anaesthesiol Scand 1996; 40: 151–5.
Kinsella J, Moffat AC, Patrick JA, Prentice JW, McArdle CS, Kenny GNC. Ketorolac trometamol for postoperative analgesia after orthopaedic surgery. Br J Anaesth 1992; 69: 19–22.
Beattie WS, Warriner CB, Etches R, et al. The addition of continuous intravenous infusion of ketorolac to a patient-controlled analgetic morphine regimen reduced postoperative myocardial ischemia in patients undergoing elective total hip or knee arthroplasty. Anesth Analg 1997; 84: 715–22.
Breisblatt WM, Stein KL, Wolfe CJ, et al. Acute myocardial dysfunction and recovery: a common occurrence after coronary bypass surgery. J Am Coll Cardiol 1990; 15: 1261–9.
Mangano DT. Biventricular function after myocardial revascularization in humans: deterioration and recovery patterns during the first 24 hours. Anesthesiology 1985; 62: 571–7.
Feldman HI, Kinman JL, Berlin JA, et al. Parenteral ketorolac: the risk for acute renal failure. Ann Intern Med 1997; 126: 193–9.
Foster DW. Diabetes mellitus.In: Wilson JD, Braunwald E, Isselbacher KJ, et al. (Eds.). Harrison’s Principles of Internal Medicine, 14th ed. New York: McGraw-Hill Inc., 1998: 2060–79.
Singh G, Ramey DR, Morfeld D, Fries JF. Comparative toxicity of non-steroidal anti-inflammatory agents. Pharmacol Ther 1994; 62: 175–91.
Kenny GNC. Potential renal, haematological and allergic adverse effects associated with nonsteroidal antiinflammatory drugs. Drugs 1992; 44: 31–7.
Perttunen K, Kalso E, Heinonen J, Salo J. I.V. Diclofenac in post-thoracotomy pain. Br J Anaesth 1992; 68: 474–80.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rapanos, T., Murphy, P., Szalai, J.P. et al. Rectal indomethacin reduces postoperative pain and morphine use after cardiac surgery. Can J Anesth 46, 725–730 (1999). https://doi.org/10.1007/BF03013906
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03013906