
Abstract
Purpose
To compared the clinical efficacy of tramadol and morphine using a patient-controlled analgesia (PCA) delivery system.
Methods
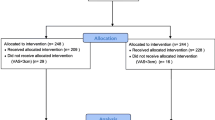
In a prospective, randomized, double blind study, we evaluated 80 adult patients scheduled for elective hip or knee arthroplasty with general inhalational anesthesia. When patients complained of pain in the recovery room, patients were randomized to receive either tramadol or morphine by titration in 30 min to achieve analgesia (VAS ≤ 4). Equivalent volumes containing either 30 mg · ml−1 tramadol or 1 mg · ml−1 morphine were used for PCA with a lockout interval of 10 min. The patients were followed six-hourly for 48 hr for VAS, satisfaction rate, analgesic dose, and side effects.
Results
Patients obtained adequate analgesia with either drug. More patients had very good satisfaction scores in the morphine group in the recovery room (43% vs 23%,P < 0.05) and at 24 hr (40% vs 20%,P < 0.05) than those in the tramadol group. More nausea was evident in the tramadol group (48% vs 11% in recovery room and 28%vs 12% in 24 hr,P < 0.05) than in the morphine group. Vomiting was also more (28% vs 5% in recovery room, 15% vs 3% in 24 hr,P < 0.05). Morphine produced more sleepiness (45% vs 23% in recovery room,P < 0.05 and 35%vs 15% in 24 hr,P < 0.05).
Conclusion
Tramadol PCA can provide effective analgesia following major orthopedic surgery provided sufficiently high doses are given for loading and by patient demand. However, the incidence of nausea/vomiting is also higher causing decreased satisfaction.
Résumé
Objectif
Comparer l’efficacité clinique du tramadol et de la morphine en utilisant un système d’analgésie contrôlée par le patient (ACP).
Méthode
Lors d’une étude prospective, randomisée et en double aveugle, nous avons évalué 80 adultes dont l’arthroplastie de la hanche ou du genou avait été prévue avec une anesthésie générale d’inhalation. À la salle de réveil, les patients répartis au hasard ont reçu, quand ils éprouvaient de la douleur, du tramadol ou de la morphine selon un dosage permettant d’atteindre l’analgésie (EVA ≤ 4) en 30 min. Des volumes équivalents contenant 30 mg · ml−1 de tramadol ou 1 mg · ml−1 de morphine ont été utilisés pour l’ACP, qui comprenait une période réfractaire de 10 min. Les patients ont été revus à toutes les six heures pendant 48 h pour l’enregistrement des scores de l’EVA, de la satisfaction, de la dose d’analgésique et des effets secondaires.
Résultats
Les patients ont obtenu une analgésie suffisante avec l’un ou i’autre médicament. Un plus grand nombre de patients a été très satisfait dans le groupe ayant reçu de la morphine à la salle de réveil (43 % vs 23 %,P < 0,05) et à 24 h (40 % vs 20 %,P < 0,05) que ceux du groupe ayant reçu le tramadol. Il y a eu davantage de nausées dans le groupe du tramadol (48 % vs 11 % dans la salle de réveil et 28 % vs 12 % à pendant les 24 premières heures, P < 0,05) que dans le groupe de la morphine. Les vomissements ont été également plus fréquents (28 % vs 5 % en salle de réveil, 15 % vs 3 % pendant les 24 premières heures, P < 0,05). La morphine a produit plus de somnolence (45 % vs 23 % en salle de réveil,P < 0,05 et 35 % vs 15 % pendant 24 h,P < 0,05).
Conclusion
LACP avec le tramadol peut assurer une analgésie efficace à la suite d’une intervention orthopédique importante, pourvu que des doses suffisamment élevées soient administrées en dose d’attaque et à la demande du patient. Cependant, l’incidence de nausées et de vomissements est aussi plus élevée avec le tramadol, ce qui en diminue l’attrait.
Article PDF
Similar content being viewed by others


References
Raffa RB, Nayak RK, Liao S, Minn FL. The mechanism(s) of action and pharmacokinetics of tramodol hydrochloride. Rev Contemp Pharmacother 1995; 6: 485–97.
Collart L, Luthy C, Dayer P. Partial inhibition of tramadol antinociceptive effect by naloxone in man. Br J Clin Pharmacol 1992; 35: 73P.
Katz WA. Pharmacology and clinical experience with tramadol in osteoarthritis. Drugs 1996; 52(Suppl3): 39–17.
Vickers MD. The efficacy of tramadol hydrochloride in the treatment of postoperative pain. Rev Contemp Pharmacother 1995; 6: 499–506.
Vickers MD, O’Flaherty D, Szekely SM, Read M, Yoshizumi J. Tramadol: pain relief by an opioid without depression of respiration. Anaesthesia 1992; 47: 291–6.
Preston KL, Jasinski DR, Testa M. Abuse potential and pharmacological comparison of tramadol and morphine. Drug Alcohol Depend 1991; 27: 7–17.
Stumer UM, Maier C, Grondt S, Veh-Schmidt B, Klaschik E, Lehmann KA. Tramadol in the management of post-operative pain: a double blind, placebo- and active drug-controlled study. Eur J Anesthesiol 1997; 14: 646–54.
Stoelting RK. Opioid agonists and antagonists.In: Stoelting RK. Pharmacology and Physiology in Anesthetic Practice. Philadelphia: JB Lippincott Company, 1987: 69–101.
Houmes R-JM, Voets MA, Verkaaik A, Erdmann W, Lachmann B. Efficacy and safety of tramadol versus morphine for moderate and severe postoperative pain with special regard to respiratory depression. Anesth Analg 1992; 74: 510–4.
Tarrdell R, Pol O, Farré M, Barrera E, Puig MM. Respiratory and analgesic effects of meperidine and tramadol in patients undergoing orthopedic surgery. Meth Find Exp Clin Pharmacol 1996; 18: 211–8.
Stubhaug A, Grimstad J, Breivik H. Lack of analgesic effect of 50 and 100 mg oral tramadol after orthopaedic surgery: a randomized, double-blind, placebo and standard active drug comparison. Pain 1995; 62: 111–8.
Amin E, Tawfik O, Elborolossy K. Tramadol hydrochloride in postoperative analgesia. A double blind comparison against butorphanol tartrate and nalbuphine hydrochloride. Pain 1990; 186(S5): 55–8.
Kupers R, Callebaut V, Debois V, et al. Efficacy and safety of oral tramadol and pentazocine for postoperative pain following prolapsed intervertebral disc repair. Acta Anesthesiol Belg 1995; 46: 31–7.
Chrubasik J, Buzina M, Schulte-Mönting J, Atanassoff P, Alon E. Intravenous tramadol for post-operative paincomparison of intermittent dose regimens with and without maintenance infusion. Eur J Anesthesiol 1992; 9: 23–8.
Lehmann KA, Kratzenberg U, Scbroeder-Bark B, Horrichs-Haermeyer G. Postoperative patient-controlled analgesia with tramadol: analgesic efficacy and minimum effective concentration. Clin J Pain 1990; 6: 212–20.
Vickers MD, Paravicini D. Comparison of tramadol with morphine for post-operative pain following abdominal surgery. Eur J Anesthesiol 1995; 12: 265–71.
De Witte J, Rietmtm GW, Vandenbroucke G, Deloof T. Post-operative effects of tramadol administered at wound closure. Eur J Anesthesiol 1998; 15: 190–5.
Ng KFJ, Tsui SL, Tang JCS, Ho ETF. Comparison of tramadol and tramadol/droperidol mixture for patientcontrolled analgesia. Can J Anaesth 1997; 44: 810–5.
Lehmann KA. Tramadol in acute pain. (French) Drugs 1997; 53(S2): 25–33.
Author information
Authors and Affiliations
Additional information
This study was carried out at the Department of Anesthesia, Show-Chwan Memorial Hospital, Changhua, Taiwan, R.O.C.
Rights and permissions
About this article
Cite this article
Pang, WW., Mok, M.S., Lin, CH. et al. Comparison of patient-controlled analgesia (PCA) with tramadol or morphine. Can J Anesth 46, 1030–1035 (1999). https://doi.org/10.1007/BF03013197
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03013197