
Abstract
Purpose
To determine whether a group of experienced clinicians can predict intensive care unit (ICU) length of stay (LOS) following cardiac surgery.
Methods
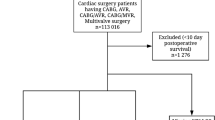
A cohort of 265 adult patients undergoing cardiacsurgery at St. Michael’s Hospital, Toronto, Ontario, between January 2, 1992, and June 26, 1992, were seen preoperatively by the clinicians participating in the study and ICU length of stay was predicted based on the clinicians’ preoperative assessment and/or information recorded in the patient’s chart.
Results
Five hundred and ten ICU length of stay predictions were obtained from a group of eight experienced clinicians (anaeslhetists/intensivists, cardiologists, nurses). The clinicians predicted the exact ICU length of stay (in days) correctly 51.2% of the time and were within ± 1 day 84.5% of the time. The clinicians correctly predicted short ICU stays (≤ 2 days) for 87.6% of the patients who had short ICU stays but only predicted long ICU stays (> 2 days) in 39.4% of the patients who had long ICU stays.
Conclusions
Experienced clinicians can predict preoperatively with a considerable degree of accuracy patients who will have short ICU lengths of stay following cardiac surgery. However, many patients who had long ICU stays were not correctly identified preoperatively. Unidentified preoperative risk factors or unanticipated intraoperative/postoperative events may be causing these patients to have longer than expected ICU stays.
Résumé
Objectif
Déterminer s’il est possible pour un groupe de cliniciens expérimentés de prédire la durée du séjour à l’unité de soins intensifs (USI) après une intervention cardiaque.
Méthodes
Une cohorte de 265 adultes opérés à l’hôpital St. Micheal de Toronto pour une chirurgie cardiaque centre le 2 janvier 1992 et le 26 juin 1992 ont été vus par les cliniciens participant à l’étude et leur durée de séjour à l’USI a été prédite sur la base de l’évaluation préopératoire et/ou des renseignements consignés au dossier.
Résultats
Cinq cent dix prédictions portant sur la durée du séjour ont été obtenues de la part de huit cliniciens expérimentés (anesthésistes/intensivistes, cardiologues, infirmières). Les cliniciens ont prédit la durée du séjour à l’USI (en jours) correctement dans 61,2% des cas et dans 84,5% à ± 1 journée près. Les cliniciens ont prédit correctement les séjours de courte durée (≤ 2 jours) pour 87,6% des courts séjours anticipés mais n’ont prédit les longs séjours (> 2 jours) que dans 39,4% des cas anticipés.
Conclusion
Il est possible pour les cliniciens expérimentés de prédire en préopératoire avec un degré de précision remarquable les courts séjours à l’USI après une chirurgie cardiaque. Par contre, plusieurs des patients ayant séjourné longuement à l’USI n’ont pas été correctement identifiés en préopératoire. Les risques préopératoires non reconnus ou des incidents per-et postopératoires imprévus peuvent causer la prolongation de certains patients à l’USI.
Similar content being viewed by others


References
Tu JV, Mazer CD, Levinton C, Armstrong PW, Naylor CD. A predictive index for length of stay in the intensive care unit following cardiac surgery. Can Med Assoc J 1994; 151: 177–85.
Naylor CD. A different view of queues in Ontario. Health Aff Millwood 1991; 10: 110–28.
Tuman KJ, McCarthy RJ, March RJ, Najafi H, Ivankovich AD. Morbidity and duration of ICU stay after cardiac surgery. A model for preoperative risk assessment. Chest 1992; 102: 36–44.
Mounsey JP, Griffith MJ, Heaviside DW, Hedley Brown A, Reid DS. Determinants of the length of stay in intensive care and in hospital after coronary artery surgery. Br Heart J 1995; 73: 92–8.
Tu JV, Jaglal SB, Naylor CD. Steering Committee of the Provincial Adult Cardiac Care Network of Ontario. Multicenter validation of a risk index for mortality, intensive care unit stay, and overall length of stay after cardiac surgery. Circulation 1995; 91: 677–84.
Pearson SD, Goulart-Fisher D, Lee TH. Critical pathways as a strategy for improving care: problems and potential. Ann Intern Med 1995; 123: 941–8.
Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982; 143: 29–36.
Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 1983; 148: 839–43.
Hähnel J, Friesdorf W, Schwilk B, Marx T, Blessing S. Can a clinician predict the technical equipment a patient will need during intensive care unit treatment? An approach to standardize and redesign the intensive care unit workstation. J Clin Monit 1992; 8: 1–6.
Hammermeister KE, Burchfiel C, Johnson R, Grover FL. Identification of patients at greatest risk for developing major complications at cardiac surgery. Circulation 1990; 82: 380–9.
Weintraub WS, Jones EL, Craver J, Guyton R, Cohen C. Determinants of prolonged length of hospital stay after coronary bypass surgery. Circulation 1989; 80: 276–84.
Author information
Authors and Affiliations
Additional information
Grant support: Dr. Tu is supported by a Health Research Personnel Devlopmenl Program Fellowship (04544) from the Ontario Ministry of Health. The results and conclusions arc those of the authors, and no official endorsement by the Ministry is intended or should be inferred.
Rights and permissions
About this article

Cite this article
Tu, J.V., Mazer, C.D. Can clinicians predict ICU length of stay following cardiac surgery?. Can J Anaesth 43, 789–794 (1996). https://doi.org/10.1007/BF03013030
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03013030