
Abstract
Purpose
The objectives of this study were: 1) to compare the estimated cardiac output (CO) by visual inspection with objective measurements by thermodilution: 2) to compare the estimated systemic vascular resistance (SVR) with objective measurements by thermodilution; and 3) to assess whether management of the patient, based on subjective values, would have differed from the management of the patient based on the objective values.
Methods
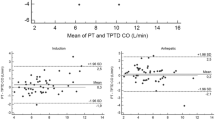
A non-randomized, prospective. blinded study was conducted at a tertiary care university hospital. Following institutional ethics approval. 35 patients undergoing cardiac surgery, with pulmonary artery catheter (PAC) monitoring, were studied. Pnor to the measurement of CO by thermodilution, but after separation from cardiac pulmonary bypass, the CO and SVR were estimated by the anaesthetist and the surgeon. Bland and Altman’s method was used for statistical analysis.
Results
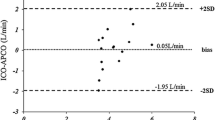
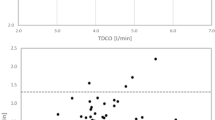
Surgeons’ estimates of CO were comparable with the objectively measured thermodilution measures: in each case (100%). the difference between the subjective estimate and the objective measurement was less than two standard deviations from the mean difference of the two methods. Anaesthetists’ estimates, by visual inspection, were also comparable with the objectively measured thermodilution values; 94.6% of cases. The surgeons’ and anaesthetists’ estimates of SVR were also comparable with the thermodilution measures in all cases. Management based on subjective values would have differed from those based on objective values in only 8.6% of cases.
Conclusion
An advantage of cardiac surgery is the ability to observe the heart and assess its performance visually This study demonstrated that estimates of CO and SVR by clinical observation are comparable with the pulmonary artery catheter s derived values.
Résumé
Objectif
Cette étude avait pour objectifs de: 1) comparer l’évaluation subjective du débit cardiaque (DC) avec la mesure objective par themnodilution; 2) comparer l’évaluation subjective de la résistance vasculaire systémique (RVS) avec la mesure objective par thermodilution; 3) vénfier si la prise en charge du patient basée sur les valeurs subjectives eut différé si elle avait été basée sur les valeurs objectives.
Méthodes
Cette étude sans randomisation, prospective et à l’aveugle a été menée dans un hôpital de soins tertiaires Sanctionnée par le comité d’éthique, elle regroupait 35 patients opérés pour une chirurgie cardiaque et monitorés par un cathéter de l’artère pulmonaire. Avant la mesure du DC par thermodilution, après l’arrêt de la circulation extracorporelle, le DC et la RVS ont été évalués par l’anesthésiste et le chirurgien La méthode statistique utilisée était celle de Bland et Altman.
Résultats
Les évaluations du DC par les chirurgiens étaient comparables aux mesures objectives obtenues par thermodilution: dans tous les cas (100%), la différence entre l’évaluation subjective et objective était mféneure à deux écarts-types de la différence moyenne entre les deux méthodes. Les valeurs des anesthésistes. obtenues visuellement, étaient aussi comparables avec les valeurs objectives obtenues par thermodilution dans 94.6% des cas Dans tous les cas, les valeurs de la RVS déterminées à la fois par les chirurgiens et les anesthésistes étaient comparables aux valeurs obtenues par thermodilution. Sur la base des valeurs subjectives, la conduite adoptée n’aurait différé que dans 8.6% des cas sur celle des valeurs objectives.
Conclusion
Un des avantages de la chirurgie cardiaque consiste à ce qu’on peut voir le coeur et ainsi déterminer sa performance. Cette étude montre que les estimations du DC et de la RVS fournies par l’observation clinique sont comparables à celles que procurent les données obtenues par le cathéténsme de l’artère pulmonaire.
Article PDF
Similar content being viewed by others
Avoid common mistakes on your manuscript.
References
Bilfinger TV, Lin C-Y, Anagnostopoulos CE.In vitro determination of accuracy of cardiac output measurements by thermal dilution. J Surg Res 1982; 33: 409–14.
Stanley TE, Reves JG. Cardiac performance monitoring.In: Miller RD (Ed.). Anesthesia, 4th ed. New York: Churchill Livingstone 1994; 1187–91.
Bazaral MG, Petre J, Novoa R. Errors in thermodilution cardiac output measurements caused by rapid pulmonary artery temperature decreases after cardiopulmonary bypass. Anesthesiology 1992;77: 31–7.
Latson TW, Whitten CW, O’Flaherty D. Ventilation, thermal noise, and errors in cardiac ouput measurements after cardiopulmonary bypass. Anesthesiology 1993; 79: 1233–43.
Stern DH, Gerson JI, Allen FB, Parker FB. Can we trust the direct radial artery pressure immediately following cardiopulmonary bypass? Anesthesiology 1985; 62: 557–61.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: 307–10.
Mangano DT. Monitoring pulmonary artery pressure in coronary-artery disease. Anesthesiology 1980; 53: 364–70.
Report by the American Society of Anesthesiologists task force on pulmonary artery catheterization. Practice guidelines for pulmonary artery catheterization. Anesthesiology 1993; 78: 380–94.
Steingrub JS, Celoria G, Vickers-Lahti M, Teres D, Bria. W. Therapeutic impact of pulmonary artery catheterization in a medical/surgical ICU. Chest 1991; 99: 1451–5.
Bashein G, Johnson PW, Davis KB, Ivey TD. Elective coronary bypass surgery without pulmonary artery catheter monitoring. Anesthesiology 1985; 63: 451–4.
Tuman KJ, McCarthy RJ, Speiss BD, et al. Effect of pulmonary artery catheterization on outcome in patients undergoing coronary artery surgery. Anesthesiology 1989; 70: 199–206.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Aye, T., Milne, B. & Ballantyne, M. Cardiac output estimation by visual inspection vs thermodilution during cardiac surgery. Can J Anaesth 44, 126–130 (1997). https://doi.org/10.1007/BF03012999
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012999