
Abstract
Purpose
To determine the efficacy and side effects of prone positioning (PP) and nitric oxide (NO) inhalation, alone, associated, or combined withiv almitrine for the treatment of hypoxaemia in severe acute respiratory distress syndrome (ARDS).
Methods
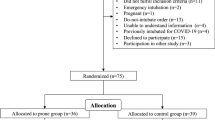
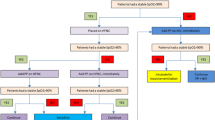
Over a period of 20 months, 27 consecutive critically ill patients with severe ARDS (Murray score > 2.5, PaO2/FiO2 < 170 after alveolar recruitment) were prospectively and randomly included. They inhaled NO for two hours at concentrations of 5 and 10 ppm for one hour each (H0–H2). One hour later, they were returned to the prone position for four hours (H3–H7). During the last two hours in this position (H5–H7), they were assigned to further inhalation of 10 ppm NO (Group B, n = 9) or to no further inhalation (Group A, n = 9). In group C (n = 9), the procedure for group B was combined with perfusion of 16 mg · kg−1 · min−1 almitrine throughout the study.
Results
Compared with control values, two hours NO inhalation improves PaO2/FiO2 and shunt effect by +28% and −9%, PP by +88% and −27%, PP + almitrine by + 132% and −28%, NO + almitrine by + 153 and −28%, PP + NO by +94% and −29%, NO + PP + almitrine by +327 and −48%. NO inhalation reduces pulmonary vascular resistance. Other haemodynamic parameters remain unchanged, whatever the treatment. NO inhalation improves PaO2/FiO2 by over 20% in 50% of the patients and PP is effective in 78% of the cases.
Conclusion
Prone Position improves PaO2/FiO2 significantly more than NO alone but less than PP+ almitrine or NO+ almitrine. The best results are obtained with the association of NO + Prone position + Almitrine.
Résumé
Objectif
Apprécier et comparer l’intérêt du décubitus ventral (DV), de l’inhalation de NO et de l’administration continue d’almitrine, seuls ou en association, dans le traitement de l’hypoxémie au cours du syndrome de détresse respiratoire aiguë (SDRA).
Méthode
Sur une période de 20 mois, 27 patients hospitalisés en réanimation avec un SDRA grave (score de Murray > 2,5, PaO2/FiO2 < 170 après recrutement alvéolaire) ont été inclus prospectivement et de manière randomisée. Ils ont bénéficié de l’inhalation de NO pendant 2 heures à la posologie de 5ppm pendant une heure puis I0ppm (H0–H2). Après une heure d’arrêt, on les a retournés 4 heures en décubitus ventral (H3–H7). De H5 à H7 un groupe A (n = 9) était traité par DV seul tandis que l’on ajoutait dans un groupe B (n = 9) l’inhalation de NO à 10 ppm. Un troisième groupe C (n = 9) bénéficiait d’une perfusion continue d’almitrine (16 mg · kg−1 · min−1) associée à cette même séquence thérapeutique.
Résultats
Par rapport à H0, 2 heures de NO améliorent le rapport PaO2/FiO2 et diminuent le shunt de +28% et −9%, le DV de +88% et −27%, les associations DV + almitrine de + 132% et −28%, NO + almitrine de +153 et −28%, DV + NO de +94% et −29%, NO + PP + almitrine de +327 et −48%. L’inhalation de NO diminue les resistances vasculaires pulmonaires. Les autres paramètres hémodynamiques restent inchangés quel que soit le traitement institué. L’inhalation de NO améliore le rapport PaO2/FiO2 de plus de 20% chez 50% des patients tandis qu’avec le même critère d’efficacité, 78% des malades sont répondeur au DV
Conclusion
Le DV s’avère plus efficace que le NO seul pour ce qui est d’améliorer le rapport PaO2/FiO2, mais moins que les associations DV + almitrine ou NO + almitrine. Les meilleurs résultats sont obtenus avec latrithérapie DV + NO + almitrine.
Article PDF
Similar content being viewed by others

References
Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet 1967; 2: 319–23.
Petty TL. Acute respiratory distress syndrome: consensus, definitions, and future directions (Editorial). Crit Care Med 1996; 24: 555–6.
DiRusso SM, Nelson LD, Safcsak K, Miller RS. Survival in patients with severe adult respiratory distress syndrome treated with high-level positive end-expiratory pressure. Crit Care Med 1995; 23: 1485–96.
Vasilyev S, Schaap RN, Mortensen JD. Hospital survival rates of patients with acute respiratory failure in modern respiratory intensive care units. Chest 1995; 107: 1083–8.
Rossaint R, Falke KJ, López F, Slama K, Pison U, Zapol WM. Inhaled nitric oxide for the adult respiratory distress syndrome. N Eng J Med 1993; 328: 399–405.
Rossaint R, Gerlach H, Schmidt-Ruhnke H, et al. Efficacy of inhaled nitric oxide in patients with severe ARDS. Chest 1995; 107: 1107–15.
Toung JD, Brampton WJ, Knighton JD, Finfer SR. Inhaled nitric oxide in acute respiratory failure in adults. Br J Anaesth 1994; 73: 499–502.
Hurford WE. Inhaled nitric oxide therapy. Curr Opin Anaesthesiol 1996; 9: 117–26.
Mizutani T, Layon AJ. Clinical applications of nitric oxide. Chest 1996; 110: 506–24.
Gerlach H, Rossaint R, Pappert D, Falke KJ. Time-course and dose-response of nitric oxide inhalation for systemic oxygenation and pulmonary hypertension in patients with adult respiratory distress syndrome. Eur J Clin Invest 1993; 23: 499–502.
Tubert V, Mansoor O, Guelon D, Schoeffler P. Prone position in acute respiratory failure: a prospective study. Anesthesiology 1994; 81: A1421.
Bigatello LM, Hurford WE, Kacmarek RM, Roberts JD Jr, Zapol WM. Prolonged inhalation of low concentrations of nitric oxide in patients with severe adult respiratory distress syndrome. Effects on pulmonary hemodynamics and oxygenation. Anesthesiology 1994; 80: 761–70.
Mourgeon E, Law-Koune JD, Lu Q et al. Inhaled NO in ARDS with and without septic shock: dose-response curves. Br J Anaesth 1995, 74: A409.
Lowson SM, Rich GF, Mc Ardle PA, Jaidev J, Morris GN. The response to varying concentrations of inhaled nitric oxide in patients with acute respiratory distress syndrome. Anesth Analg 1996; 82: 574–81.
Puybasset L, Rouby JJ, Mourgeon E, et al. Inhaled nitric oxide in acute respiratory failure: dose-response curves. Intensive Care Med 1994; 20: 319–27.
Winkelmann BR, Hertrich F, Trenk D, Jeanniot JP, Ansquer JC. Pharmacokinetics and pharmacodynamics of almitrine in man following single and repeated administration. Eur Resp J 1988; S1: 148s.
Roupie E, Wysocki M, Langeron O, et al. Effects of inhaled nitric oxide on oxygenation and hemodynamic parameters in the acute respiratory distress syndrome (ARDS). Responders versus non-responders? (French) Réan Urg 1994; 1: 671.
Mira JP, Monchi M, Brunet F, Fierobe L, Dhainaut JF, Dinh-Xuan AT. Lack of efficacy of inhaled nitric oxide in ARDS. Intensive Care Med 1994; 20: 532.
Puybasset L, Rouby J-J, Mourgeon E, et al. Factors influencing cardiopulmonary effects of inhaled nitric oxide in acute respiratory failure. Am J Respir Crit Care Med 1995; 152: 318–28.
Reyes A, Roca J, Rodriguez-Roisin R, Torres A, Ussetti P, Wagner P. Effect of almitrine on ventilation-perfusion distribution in adult respiratory distress syndrome. Am Rev Respir Dis 1988; 137: 1062–7.
Reyes A, López-Messa JB, Alonso P. Almitrine in acute respiratory failure. Effects on pulmonary gas exchange and circulation. Chest 1987; 91: 388–93.
Payen D, Gatecel C, Plaisance P. Almitrine effect on nitric oxide inhalation in adult respiratory distress syndrome. Lancet 1993; 341: 1664.
Wysocki M, Delclaux C, Roupie E, et al. Additive effect on gas exchange of inhaled nitric oxide and intravenous almitrine bismesylate in the adult respiratory distress syndrome. Intensive Care Med 1994; 20: 254–9.
Lu Q, Mourgeon E, Law-Koune JD, et al. Doseresponse curves of inhaled nitric oxide with and without intravenous almitrine in nitric oxide-responding patients with acute respiratory distress syndrome. Anesthesiology 1995; 83: 929–43.
Law-Koune JD, Roche S, Mourgeon E, et al. Increasing concentrations of inhaled NO in combination with almitrine in patients with ARDS. Am J Respir Clin Care Med 1995; 151: A76.
Albert RK, Leasa D, Sanderson M, Robertson HT, Hlastala MP. The prone position improves arterial oxygenation and reduces shunt in oleic-acid-induced acute lung injury. Am Rev Respir Dis 1987; 135: 628–33.
Pelosi P, Croci M, Calappi E, et al. Prone positioning improves pulmonary function in obese patients during general anesthesia. Anesth Analg 1996; 83: 578–83.
Krayer S, Rehder K, Vettermann J, Didier EP, Ritman EL. Position and motion of the human diaphragm during anesthesia-paralysis. Anesthesiology 1989; 70: 891–8.
Priolet B, Tempelhoff G, Millet J, et al. Mechanical ventilation in prone position: computerized tomographic evaluation of its efficacity for treatment of pulmonary condensations. (French) Réan Urg 1993; 2: 81–5.
Gattinoni L, Pelosi P, Vitale G, Pesenti A, D’Andrea L, Mascheroni D. Body position changes redistribute lung computed tomographic density in patients with acute respiratory failure. Anesthesiology 1991; 71: 15–23.
Chatte G, Sab J-M, Dubois J-M, Sirodot M, Gaussorgues P, Robert D. Prone position in mechanically ventilated patients with severe acute respiratory failure. Am J Respir Crit Care Med 1997; 155: 473–8.
Dubois JM, Gaussorgues P, Sirodot M, et al. Prone position dependency in severely hypoxic patients. Int Care Med 1992; 18: S43.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Gillart, T., Bazin, J.E., Cosserant, B. et al. Combined nitric oxide inhalation, prone positioning and almitrine infusion improve oxygenation in severe ARDS. Can J Anaesth 45, 402–409 (1998). https://doi.org/10.1007/BF03012574
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012574