
Abstract
Purpose
The gradient between temperatures measured at different body sites is not constant; one factor which will change this gradient is rapid changes in body temperature. Measurement of this gradient was done in patients undergoing rapid changes in body temperature to establish the best site to measure temperature and to compare two brands of commercial tympanic thermometers.
Method
A total of 228 sets of temperatures were measured from probes in the oesophagus, rectum, and axilla and from two brands of tympanic thermometer and compared with pulmonary artery (PA) temperature in 18 adults during cardiac surgery.
Results
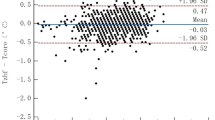
Measurements from the oesophageal site was closest to PA readings (mean difference 0.0 ± 0.5°C) compared with IVAC tympanic thermometer (mean difference −0.3 ± 0.5°C), Genius tympanic thermometer (mean difference −0.4 ± 0.5°C), axillary (mean difference 0.2 ± 1.0dgC) and rectal (mean difference −0.4 ± 1,0°C) readings. When data during cooling were analysed separately, all sites had similar gradients from PA except for rectal, which was larger. On rewarming, oesophageal readings were closest to PA readings; tympanic readings were closer to PA than were rectal or axillary readings. Readings from the two brands of tympanic thermometer were equivalent.
Conclusion
Oesophageal temperature is more accurate and will reflect rapid changes in body temperature better than tympanic, axillary, or rectal temperature. When oesophageal temperature cannot be measured, tympanic temperature done by a trained operator should become the reading of choice.
Résumé
Objectif
Le gradient entre les mesures de température réalisées à différents endroits du corps n’est pas constant; les changements rapides de la température corporelle représentent un des facteurs modifiant ce gradient. Ce dernier a été mesuré chez des patients subissant des changements rapides de la température corporelle dans le but d’identifier le meilleur endroit où mesurer la température et dans le but de comparer deux marques de thermomètre tympanique sur le marché.
Méthode
Un total de 228 groupes de mesures de la température ont été obtenues à partir des sites oesophagien, rectal, axillaire et tympaniqué (deux marques de thermomètre) et ont été comparés aux mesures réalisées dans l’artère pulmonaire chez 18 adultes subissant une chirurgie cardiaque.
Résultats
Les mesures oesophagiennes étaient les plus proches de celles de l’artère pulmonaire (différence moyenne (0,0 ± 0,5°C), comparativement aux mesures tympaniques par thermomètre IVAC(−0,3 ± 0,5°C) et Genius (−0,4 ± 0,5°C), aux mesures axillaires (0,2 ± 1°C) et aux mesures rectales (−0,4 ± 1°C). Lorsque les mesures durant le refroidissement étaient analysées séparément, tous les sites démontraient des gradients analogues par rapport à l’artère pulmonaire, sauf le rectum qui démontrait un gradient plus considérable. Lors du réchauffement, les mesures oesophagiennes étaient plus proches de celles de l’artère pulmonaire, suivies des mesures tympaniques, avant les mesures axillaires ou rectales. Les lectures obtenues avec les deux marques de thermomètre tympaniqué se sont avérées équivalentes.
Conclusion
La température oesophagienne est plus précise et reflète mieux les changements rapides de température corporelle que les sites tympaniqué, axillaire ou rectal. Lorsqu’on ne peut mesurer la température oesophagienne, la mesure tympaniqué réalisée par un opérateur entraîné devrait être la mesure de choix.
Article PDF
Similar content being viewed by others


References
Cork RC, Vaughan RW, Humphrey LS. Precision and accuracy of intraoperative temperature monitoring. Anesth Analg 1983; 62: 211–4.
Eichnn LW, Berger AR, Ruder B, Buckaroo WH. Comparison of intracardiac and intravascular temperatures with rectal temperatures in man. J Clin Invest 1951; 30: 353–9.
Severinghaus JW. Temperature gradients during hypothermia. Ann NY Acad Sci 1959; 80: 515–21.
Molnar GW, Read RC. Studies during open-heart surgery on the special characteristics of rectal temperature. J Appl Physiol 1974; 36: 333–6.
Hayward JS, Eckerson JD, Kemna D. Thermal and cardiovascular changes during three methods of resuscitation from mild hypothermia. Resuscitation 1984; 11: 21–33.
Shiraki K, Konda N, Sagawa S. Esophageal and tympanic temperature responses to core blood temperature changes during hyperthermia. J Appl Physiol 1986; 61: 98–102.
Whitby JD, Dunkin LJ. Cerebral, oesophageal and nasopharyngeal temperatures. Br J Anaesth 1971; 43: 673–6.
Mariak Z, Bondya Z, Piekarska M. The temperature within the circle of Willis versus tympanic temperature in resting normothermic humans. Eur J Appl Physiol. 1993; 66: 518–20.
Whitby JD, Dunkin LJ. Temperature differences in the esophagus. Br J Anaesth 1968; 40: 991–5.
Kresovich-Wendler, Levitt MA, Yearly L. An evaluation of clinical predictors to determine need for rectal temperature measurement in the emergency department. Am J Emerg Med 1989; 7: 391–4.
Terndrup TE, Allegro JR, Kealy JA. A comparison of oral, rectal, and tympanic membrane-derived temperature changes after ingestion of liquids and smoking. Am J Emerg Med 1989; 7: 150–4.
Nichols GA, Ruskin MM, Glor BAK, Kelly WH. Oral, axillary, and rectal temperature determinations and relationships. Nurs Res 1966; 15: 307–10.
Pugh Davies S, Kassab JY, Thrush AJ, Smith PHS. A comparison of mercury and digital clinical thermometers. J Adv Nurs 1986; 11: 535–43.
Johnson KJ, Bhatia P, Bell EF. Infrared thermometry of newborn infants. Pediatrics 1991; 87: 34–8.
Baker MA, Stocking RA, Meehan JP. Thermal relationship between tympanic membrane and hypothalamus in conscious cat and monkey. J Appl Physiol 1972; 32: 739–42.
Kenney RD, Fortenberry JD, Surratt SS, Ribbeck BM, Thomas WJ. Evaluation of an infrared tympanic membrane thermometer in pediatrie patients. Pediatrics 1990; 85: 854–8.
Ferrara-Love R. A comparison of tympanic and pulmonary artery measures of core temperatures. J Post Anesth Nurs 1991; 6: 161–4.
Milewski A, Ferguson KL, Terndrup TE. Comparison of pulmonary artery, rectal, and tympanic membrane temperatures in adult intensive care unit patients. Clin Pediatr 1991; 30(Suppl): 13–6.
Shinozaki T, Deane R, Perkins FM. Infrared tympanic thermometer: evaluation of a new clinical thermometer. Crit Care Med 1988; 16: 148–50.
Jakobsson J, Nilsson A, Carlssen L. Core temperature measured in the auricular canal: comparison between four different tympanic thermometers. Acta Anesthiol Scand 1992; 36: 819–24.
Lattavo K, Britt J, Dobal M. Agreement between measures of pulmonary artery and tympanic temperatures. Res Nurs Health 1995; 18: 365–70.
Heidenreich T, Giuffre M, Doorley J. Temperature and temperature measurement after induced hypothermia. Nurs Res 1992; 41: 296–300.
Nierman DM. Core temperature measurement in the intensive care unit. Crit Care Med 1991; 19: 818–23.
Klein DG, Mitchell C, Petrinec A, et al. A comparison on pulmonary artery, rectal, and tympanic membrane temperature measurement in the ICU. Heart Lung 1993; 22: 435–41.
Romano MJ, Fortenberry JD, Autrey E, et al. Infrared tympanic thermometry in the pediatric intensive care unit. Crit Care Med 1993; 21: 1181–5.
Erickson RS, Kirklin SK. Comparison of ear-based, bladder, oral, and axillary methods for core temperature measurement. Crit Care Med 1993; 21: 1528–34.
White N, Baird S, Anderson DL. A comparison of tympanic thermometer readings to pulmonary artery catheter core temperature readings. Appl Nurs Res 1994; 7: 165–9.
Erickson RS, Meyer LT. Accuracy of infrared ear thermometry and other temperature methods in adults. Am J Crit Care 1994; 3: 40–54.
Stone JG, Young WL, Smith CR, et al. Do standard monitoring sites reflect true brain temperature when profound hypothermia is rapidly induced and reversed? Anesthesiology 1995; 82: 344–51.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was funded in part by ALARIS Medical Systems Inc. (formerly known as IVAC Inc.).
Rights and permissions
About this article
Cite this article
Robinson, J., Charlton, J., Seal, R. et al. Oesophageal, rectal, axillary, tympanic and pulmonary artery temperatures during cardiac surgery. Can J Anaesth 45, 317–323 (1998). https://doi.org/10.1007/BF03012021
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012021