
Abstract
Purpose
The concept of balanced analgesia suggests that a combination of analgesic drugs may enhance analgesia and reduce side effects after surgery. This study evaluated the effect of the combination of propacetamol (Prodafalgan) and ketoprofen (Profenid) after surgery of a hemiated disc of the lumbar spine.
Methods
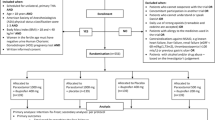
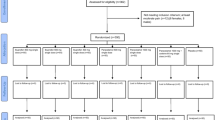
After randomization. 60 patients received: placebo (group 1); 2 g propacetamol (group 2); 50 mg ketoprofen (group 3); or a combination of 2 g propacetamol and 50 mg ketoprofen (group 4). Drugs were administered every six hours for two days after surgery. The patients used morphine with patient controlled analgesia pumps (bolus 1mg; lock out time 10 min) and were evaluated with a visual analogue scale (VAS) at rest and movement every six hours for two days. Side effects were noted.
Results
The patient characteristics and surgery were identical for each of the four groups. The VAS scores throughout the study were lower in group 4 than in groups 1, 2 and 3 both at rest (P < 0.05) and on movement (P < 0.01). The cumulative dose of morphine at 48 hr was lower in group 4 than in group 1 (23.4 ± 5 mg vs 58.9 ± 9 mg; P < 0.01) or group 2 (23.4 ± 5 mg vs 43.4 ± 6.6 mg; P < 0.05) and similar to that in group 3 (34.2 ± 4.5 mg). The incidence of side effects was similar in all groups.
Conclusion
The combination of propacetamol and ketoprofen reduced pain scores both at rest and on movement. The drug combination did not reduce the morphine consumption and incidence of side effects.
Résumé
But
Le concept d’analgésie balancée suggère que I’association de drogues analgésiques en postopératoire peut permettre d’améliorer I’analgésie et réduire les effets secondaires. Cette étude a évalué I’intérêt d’une association de propacetamol (Prodafalgan) et de ketoprofen (Profenid) pour I’analgésie après chirurgie d’une hernie discale lombaire.
Méthodes
Après randomisation 60 patients ont reçu: un placebo (groupe 1); 2 g de propacetamol (groupe 2); 50 mg de ketoprofen (groupe 3); où I’association de 2 g de propacetamol et 50 mg de ketoprofen (groupe 4). Les produits analgésiques ont été administrés toutes les six heures pendant 48 h. Les patients utilisaient de la morphine grâce à une pompe d’analgésie autocontrôlée pendant 48 h (bolus 1mg; période réfractaire 10 mm) et la douleur était évaluée par échelle visuelle analogique toutes les six heures au repos et au mouvement. Les effets secondaires étaient notés toutes les six heures.
Resultats
Les patients et la chirurgie étaient similaires dans les quatre groupes. Les scores d’EVA etaient plus bas pendant les 48 heures de I’étude dans le groupe 4 par rapport à ceux des groupes 1, 2 et 3 au repos (P < 0.05) comme au mouvement (P < 0.01). Les doses cumulées de morphine étaient significativement plus basses à 48 h dans le groupe 4 par rapport au groupe 1 (23.4 ± 5 mg vs 58.9 ± 9 mg; P < 0.01). groupe 2 (23.4 ± 5 mgvs 43.4 ± 6.6 mg; P < 0.05) et pas significativement différentes de celles du groupe 3 (34.2 ± 4.5 mg). L’incidence des effets secondaires était similaire dans tous les groupes.
Conclusion
L’association de propacetamol et ketoprofen a réduit les scores de douleur au repos et au mouvement par rapport aux groupes traités par une seule drogue analgésique. Lassociation propacetamol-ketoprofen n’a pas significativement réduit la consommation de morphine et les effets secondaires Iiés à la morphine.
Article PDF
Similar content being viewed by others

References
Kehlet H, Dahl JB. The value of “multimodal or “balanced analgesia” in postoperative treatment. Anesth Analg 1993;77: 1048–56.
Dahl JB, Kehlet H. Non-steroidal anti-inflammatory drugs: rationale for use in severe postoperative pain. Br J Anaesth 1991;66: 703–12.
Dahl JB, Rosenberg J, Dirkes WE, Mogensen T, Kehlet H. Prevention of postoperative pain by balanced analgesia. Br J Anaesth 1990; 64: 518–20.
Rawal N. Analgesia technique and post-operative morbidity. Eur J Anaesthesiol 1995; 10: 47–52.
Honoré P, Buritova J, Besson J-M. Aspirin and acetaminophen reduced both Fos expression in rat lumbar spinal cord and inflammatory signs produced by carrageenin inflammation. Pain 1995; 63: 365–75.
Piletta P, Porchet HC, Dayer P. Central analgesic effect of acetaminophen but not of aspirin. Clin Pharmacol Ther 1991;49: 350–4.
Ferreira SH, Moncada S, Vane JR. Prostaglandins and the mechanism of analgesia produced by aspirin-like drugs. Br J Pharmacol 1973; 49: 86–97.
Vane JR. Inhibition of prostaglandin synthesis as a mechanism of action for aspirin-like drugs. Nature New Biology 1971; 231: 232–5.
McCormack K. Non-steroidal anti-inflammatory drugs and spinal nociceptive processing. Pain 1994; 59: 9–43.
Willer J-C, De Broucker T, Bussel B, Roby-Brami A, Harrewyn J-M. Central analgesic effect of ketoprofen in humans: electrophysiological evidence for a supraspinal mechanism in a double-blind and cross-over study. Pain 1989; 38: 1–7.
Flower RJ, Vane JR. Inhibition of prostaglandin synthetase in brain explains the anti-pyretic activity of paracetamol (4-aminodophenol). Nature 1972; 240: 410–11.
Skjelbred P, Lekken P, Skoglund LA. Postoperative administration of acetaminophen to reduce swelling and other inflammatory events. Current Therapeutic Research1984; 35: 377–85.
Delbos A, Boccard E. The morphine-sparing effect of propacetamol in orthopedic postoperative pain. J Pain Symptom Manage 1995; 10: 279–90.
Hans P, Brichant JF, Bonhomme V, Triffaux M. Analgesic efficiency of propacetamol hydrochlorid after lumbar disc surgery. Acta Anaesth Belg 1993; 44: 129–33.
Etches RC, Warriner CB, Badner N, et al. Continuous intravenous administration of ketorolac reduces pain and morphine consumption after total hip or knee arthroplasty. Anesth Analg1995; 81: 1175–80.
Grass JA, Sakima NT, Valley M, et al. Assessment of ketorolac as an adjuvant to fentanyl patient-controlled epidural analgesia after radical retropubic prostatectomy. Anesthesiology 1993; 78: 642–8.
Liu SS, Carpenter RL, Mackey DC, et al. Effects of perioperative analgesic technique on rate of recovery after colon surgery. Anesthesiology, 1995; 83: 757–65.
Bardram L, Funch-Jensen P, Jensen P, Crawford ME, Kehlet H. Recovery after laparoscopic colonic surgery with epidural analgesia, and early oral nutrition and mobiblisation. Lancet 1995; 345: 763–4.
Poisson-Salomon AS, Brasseur L, Lory C, Chauvin M, Durieux P, et al.groupe de pilotage. Audit of postoperative pain management in University Hospital. (French) Nouvelle Presse Med 1996; 25: 1013–7.
Nègre I, Fletcher D, Barbin C, et al. Contrôle qualité et douleur aiguë postopératoire. Ann Fr Anesth Réanim (Abstract) 1996; 15: R167.
Tjølsen A, Lund A, Hole K. Antinociceptive effect of paracetamol in rats is partly dependent on spinal serotoninergic systems. Eur J Pharmacol 1991; 193: 193–201.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Fletcher, D., Nègre, I., Barbin, C. et al. Postoperative analgesia withiv propacetamol and ketoprofen combination after disc surgery. Can J Anaesth 44, 479–485 (1997). https://doi.org/10.1007/BF03011934
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03011934