
Abstract
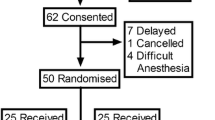
This study was undertaken to analyze the effect of posture on the spread of hyperbaric bupivacaine in pregnant women using a combined spinal extradural technique, and to assess the quality of analgesia provided by 10 mg bupivacaine when using this technique. Fifty parturients undergoing elective Caesarean section under regional anaesthesia were randomly allocated to receive 2.0 ml hyperbaric bupivacaine 0.5% in either the sitting or left lateral position. Spinal injection was performed with a 27 gauge, 120 mm long spinal needle using a single space combined spinal extradural technique. The onset time to analgesia at T4, and grade 3 motor block was on average 7.7 min and 6.9 min respectively in the lateral group, compared with 10.8 min (P < 0.05) and 9.4 min (P < 0.05) in the sitting group. Nine women in the sitting group and one woman (P < 0.05) in the lateral group required epidural supplementation. Hypotension occurred in 48% of the parturients in the lateral group and in 13% (P < 0.05) of the parturients in the sitting group. Nausea was noted in 61% of the parturients in the lateral group and in 22% (P < 0.05) of the parturients in the sitting group. There was no difference between the two groups in neonatal outcome. Overall, the position of the patient during induction of spinal anaesthesia does influence the rate of onset of analgesia and motor blockade. Injection of 10 mg hyperbaric bupivacaine in the sitting position would not provide adequate analgesia for Caesarean section when using a single space combined spinal extradural technique.
Résumé
Cette étude vise à évaluer: 1) l’effet de la position sur la dispersion, chez la parturiente, de la bupivacaine pendant une technique combinant la rachianesthésie à l’épidurale, 2) la qualité de l’anesthésie produite par bupivacaine 10 mg avec cette technique. Cinquante parturientes programmées pour césarienne sont réparties au hasard pour recevoir de la bupivacaine hyperbare 0.5% 2.0 ml en position latérale gauche (groupe latéral) ou assise (groupe assis). L’injection rachidienne est réalisée avec une aiguille 27G de 120 mm de longueur insérée dans l’espace choisi pour la technique combinée rachi- épidurale. La vitesse d’installation jusqu’à l’analgésie au niveau T4, et le bloc moteur de grade 3 sont en moyenne de 7.7 min et 6.9 min respectivement dans le groupe latéral, comparativement à 10.8 (P < 0.05) et 9.4 min dans le groupe assis (P < 0.05). Neuf patientes du groupe assis et une seule (P < 0.05) du groupe latéral ont besoin d’un supplément épidural. De l’hypotension survient dans 48% du groupe latéral et dans 13% du groupe assis (P < 0.05). On retrouve de la nausée dans 61% du groupe latéral et dans 22% du groupe assis (P < 0.05). L’état du nouveau- né est identique dans les deux groupes. En général, la position de la parturiente pendant l’induction de la rachianesthésie a une influence sur la rapidité d’installation de l’analgésie et du bloc moteur. L’injection de bupivacaïne hyperbare 10 mg en position assise ne produit pas une analgésie satisfaisante pour la césarienne quand on utilise la technique combinée rachi-épidurale administrée dans le même espace.
Article PDF
Similar content being viewed by others

References
Kestin IG. Spinal anaesthesia in obstetrics. Br J Anaesth 1991; 66: 596–607.
Russell IF. Effect of posture during the induction of sub arachnoid analgesia for Caesarean section: right v. left lat eral. Br J Anaesth 1987; 59: 342–6.
Russell IF. Posture and isobaric subarachnoid anaesthesia. Anaesthesia 1984; 39: 865–7.
Russell IF. Spinal anaesthesia for Caesarean section (Let ter). Anaesthesia 1988; 43: 704–5.
Santos A, Pedersen H, Finster M, Endström M. Hyperbaric bupivacaine for spinal anesthesia in cesarean section. Anesth Analg 1984; 63: 1009–13.
Carrie LES, O’Sullivan G. Subarachnoid bupivacaine 0.5% for Caesarean section. Eur J Anaesthesiol 1984; 1: 275–83.
Coates MB. Combined subarachnoid and epidural tech niques (Letter). Anaesthesia 1982, 37: 89–90.
Bromage PR. A comparison of hydrochloride and carbon dioxide salts of lidocaine and prilocaine in epidural anal gesia. Acta Anaesthesiol Scand 1965; (suppl. XVI): 55–69.
Eldor J, Guedj P, Gozal Y Combined spinal-epidural anesthesia using the CSEN (Letter). Anesth Analg 1992; 74: 169–70.
Lowson SM, Brown J, Wilkins CJ. Influence of the lum bar interspace chosen for injection on the spread of hyper baric 0.5% bupivacaine. Br J Anaesth 1991; 66: 465–8.
DeSimone CA, Norris MC, Leighton BL, Epstein RH, Palmer C. Spinal anesthesia for cesarean section and post partum tubal ligation. Anesthesiology 1989; 71: A837.
Randalls B, Broadway JW, Browne DA, Morgan BM. A comparison of four subarachnoid solutions in a needle- through-needle technique for elective Caesarean section. Br J Anaesth 1991; 66: 314–8.
Moir DD. Local anaesthetic techniques in obstetrics. Br J Anaesth 1986; 58: 747–59.
Manchikanti L, Hadley C, Markwell SJ, Colliver JA. A retrospective analysis of failed spinal anesthetic attempts in a community hospital. Anesth Analg 1987; 66: 363–6.
Rawal N, Schottin J, Wesström G. Epidural versus com bined spinal extradural block for cesarean section. Acta Anaesthesiol Scand 1988; 32: 61–6.
Datta S, Alper MH, Ostheimer GW, Weiss JB. Method of ephedrine administration and nausea and hypotension dur ing spinal anesthesia for cesarean section. Anesthesiology 1982; 56: 68–70.
Corke BC, Datta S, Ostheimer GW, Weiss JB, Alper MH. Spinal anaesthesia for Caesarean section. The influence of hypotension on neonatal outcome. Anaesthesia 1982; 37: 658–62.
Kang YG, Abouleish E, Caritis S. Prophylactic intrave nous ephedrine infusion during spinal anesthesia for cesa rean section. Anesth Analg 1982; 61: 839–42.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Patel, M., Samsoon, G., Swami, A. et al. Posture and the spread of hyperbaric bupivacaine in parturients using the combined spinal epidural technique. Can J Anaesth 40, 943–946 (1993). https://doi.org/10.1007/BF03010097
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03010097