
Abstract
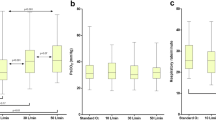
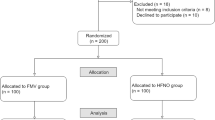
This randomized controlled trial compared the compliance of a blow-by oxygen method with the standard face mask by children recovering from anaesthesia. The rate at which a face mask was rejected when applied to infants and children in PACU was compared with that of a proposed “hose” method. The efficacy of the “hose” as a method of oxygen supplementation in children at low and high risk for developing postoperative hypoxaemia was also compared with the face mask. Using a Nellcor N-200 pulse oximeter, 66 infants and children (mean age 2.3 yr, range 2 mo-6yr) were continuously monitored for 30 min upon arrival in the PACU. Patients were randomized to receive oxygen supplementation with either the face mask or the proposed “hose“ method. The results showed a greater than 80 per cent rejection of the face mask in contrast to 100 per cent compliance with the “hose” method. The SaO2 measurements following 5, 15 and 30 min of O2 supplementation with the hose were all significantly higher than the SaO2 measurements obtained on room air upon arrival to the PACU. Patients with pre-existing cardiopulmonary disease had a 20 per cent incidence of arterial oxygen desaturation upon arrival to the PACU versus 2.1 per cent of patients with no pre-existing disease. It is concluded that the “hose” is associated with high patient compliance and is effective in the PACU in increasing the SaO2 in children at low or high risk of developing postoperative hypoxaemia.
Résumé
Cette étude randomisée et contrôlée compare la compliance de la méthode d’ « insuflation » de l’oxygène avec celle du masque facial standard pour les enfants en période de réveil de l’anesthésie. Le taux de rejet du masque, quand appliqué aux bébés et enfants à l’unité de soins postanesthésiques. a été comparé avec celui proposé et appelé la méthode par « insuflation ». L’efficacité de cette dernière méthode pour l’oxygénation des enfants à risque faible ou élevé de développer de l’hypoxémie postopératoire a aussi été comparée avec la méthode du masque facial. Utilisant le Nellcor N-200 saturomètre de pouls 66 bébés et enfants (moyenne d’âge 2,3 ans, écart 2 mois-6 ans) ont été surveillés continuellement pour 30 minutes dès l’arrivée à l’unité des soins postanesthésiques. Les patients furent randomisés afin de recevoir de l’oxygène par l’une ou l’autre des méthodes. Les résultats ont démontré un plus grand taux de rejet du masque facial (80 pour cent) et une compliance de 100 pour cent à la méthode d’ « insuflation ». Les mesures de la SaO2 après 5, 15 et 30 minutes de supplément d’oxygène par « insuflation » étaient aussi significativement supérieures aux saturations à mesurer à l’arrivée à l’unité des soins postanesthésiques avec l’air libre. Les patients ayant des maladies cardiopulmonaires pré-existantes avaient une incidence de 20 pour cent de désaturation artérielle dès leur arrivée à l’unité des soins postanesthésiques versus 2,1 pour cent chez les patients qui étaient exempts de maladie pré-existante. On conclut que la méthode d’ « insuflation » est associée avec une plus grande acceptation par le patient et a été efficace afin d’augmenter la saturation SaO2 à l’unité des soins postanesthésiques chez les enfants ayant un risque faible ou élevé de développer de l’hypoxémie postopératoire.
Article PDF
Similar content being viewed by others

References
Nunn JF, Payne P. Hypoxaemia after general anaesthesia. Lancet 1962; 2: 631–2.
Marshall BE, Wyche MQ Jr. Hypoxemia during and after anesthesia. Anesthesiology 1972; 37: 178–209.
Selim D, Markello R, Baker JM. The relationship of ventilation to diffusion hypoxia. Anesth Analg 1970; 49: 437–40.
Sheffer L, Steffenson JL, Birch AA. Nitrous oxide diffusion hypoxia in patients breathing spontaneously. Anesthesiology 1972; 37: 436–9.
Tyler IL, Tantisira B, Winter PM, Motoyama EK. Continuous monitoring of arterial oxygen saturation with pulse oximctry during transfer to the recovery room. Anesth Analg 1985; 64: 1108–12.
Meiklejohn BH, Smith G, Elling AE, Hindocha N. Arterial oxygen desaturation during postoperative transportation: the influence of operation site. Anaesthesia 1987; 42: 1313–5.
Vegfors M, Cedarholm I, Lennmarken C, Liofstriom JB. Should oxygen be administered after laparoscopy in healthy patients? Acta Anaesthesiol Scand 1988; 32: 350–2.
Smith DC, Crul JF. Early postoperative hypoxia during transport. Br J Anaesth 1988; 61: 625–7.
Brown MD, Kallar S. Hypoxemia in children following general anesthesia in the ambulatory surgery center. Anesthesiology 1985; 63: A460.
Motoyama EK, Glazener CH. Hypoxemia after general anesthesia in children. Anesth Analg 1986; 65: 267–72.
Soliman IE, Patel RI, Ehrenpreis MB, Hannallah RS. Recovery scores do not correlate with postoperative hypoxemia in children. Ancsth Analg 1987; 67: 53–6.
Desoto H, Patel RI, Soliman IE, Hannallah RS. Changes in oxygen saturation following general anesthesia in children with upper respiratory infection signs and symptoms undergoing otolaryngological procedures. Anesthesiology 1988; 68: 276–9.
Vijayakumar HR, Metriyakool K, Jewell MR. Effect of 100 per cent oxygen and a mixture of oxygen and air on oxygen saturation in the immediate postoperative period in children. Ancsth Analg 1987; 66: 181–4.
Patel R, Norden J, Hannallah RS. Oxygen administration prevents hypoxemia during post-anesthetic transport in children. Anesthesiology 1988; 69: 616–8.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Amar, D., Brodman, L.E., Winikoff, S.A. et al. An alternative oxygen delivery system for infants and children in the post-anaesthesia care unit. Can J Anaesth 38, 49–53 (1991). https://doi.org/10.1007/BF03009163
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03009163