
Summary
Innovar, a mixture of phentanyl and droperidol (0.CI2 mg./c.c. and 1 mg./c.c. respectively), was used to supplement nitrous oxide and other forms of anaesthesia. In contrast to the techniques of neuroleptanalgesia, small doses of thiopen-tone were used for induction and as a hypnotic when required. With this technique, the dosage of Innovar could be reduced, minimizing side-effects.
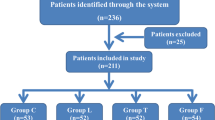
Innovar was given to 230 patients. In 24 it was used to provide sedation during regional anaesthesia; nine bronchoscopies were done using a combination of thiopentone, Innovar, and topical anaesthesia, with superior results.
The remaining 197 patients received Innovar to supplement nitrous-oxide anaesthesia. The dosages required were similar in curarized patients on controlled ventilation and patients breathing spontaneously. Innovar: induced a marked slowing of the respiration, although most patients were able to maintain their alveolar ventilation by a corresponding increase in tidal volume; only a mild respiratory acidosis (averagepCO2, 49 mm. Hg) was found in 10 patients after an average of 165 minutes of anaesthesia.
Although the technique described lacked the flexibility of inhalation anaesthesia, certain advantages deserve further consideration. Among them, the possibility to intubate the patient without loss of reflexes and without relaxants, the lack of circulatory depression, the; possible benefit of a mild adrenergic blockade, the rapid return of responsiveness, and the calm postoperative period with reduced drug requirements were particularly noticed. At the same time, the postoperative “neurolepsis” may require a closer supervision of the patient.
None of the three postoperative deaths in this series can be related to Innovar; however, one circulatory collapse occurred within the possible duration of action of droperidol.
Although the term “neuroleptanalgesia” describes the uniqlue effect of this combination of drugs, the justification to apply the term to a technique of general anaesthesia is questioned. The use of Innovar within the framework of the present concept of anaesthesia has shown promising results and shjould be actively continued.
Résumé
Nous avons employé l’innovar, un mélange de phentanyl et de droperidol (0.02 mg./ml. et 1 mg./ml. respectivement ) pour compléter l’anesthésie au pro-toxyde d’azote et aux autre mélanges d’agents. Contrairement à ce qui se fait lorsque les techniques de neuroleptanalgésie sont utilisées, nous avons employé de petites doses de thiopentone pour faire l’induction et comme hypnotique selon le besoin. De cette façon, il est possible de réduire la quantité d’innovar, ainsi que les effets secondaires.
Nous avons donné dé l’innovar à 230 malades. Chez 24 malades, nous l’avons employé comme sédatif au cours d’anesthésies régionales; nous avons pratiqué 9 bronchoscopies en employant un mélange de thiopentone, d’innovar et d’anesthésie locale et avons obtenu des résultats de toute première qualité.
Les 197 autres malades ont reçu de l’innovar pour compléter une anesthésie au protoxyde d’azote. Il nous a fallu donner les mêmes quantités aux malades curarisés dont la ventilation était contrôlée qu’aux malades qui respiraient spontanément. L’innovar produit un ralentissement marqué de la respiration; toutefois la plupart des malades ont réussi à maintenir leur ventilation alvéolaire en augmentant leur air courant; nous avèns trouvé une très légèere acidose respiratoire (pCO2 = 49) chez dix malades après 165 minutes d’aneisthésie.
Bien que cette technique anesthésique n’ait pas la souplesse de l’anesthésie par inhalation, nous attirons l’attentioln sur certains avantages. Parmi ces avantages, signalons la possibilité d’intuber le malade sans qu’il ait perdu ses réflexes et sans qu’il ait reçu des substances curarisantes, l’absence de collapse circulatoire, l’avantage possible d’un léger blocage adrénergique, un retour rapide à la capacité de répondre et une période postopératoire calme où il faut donner moins de médicaments. En même temps, la neurolepsie post-opérjatoire peut exiger une surveillance plus étroite du malade.
Aucune des trois mortalités post-opératoirek survenues au cours de cette série n’est attribuable à l’innovar; un collapse circulatoire est survenu alors que Faction du dropéridol se faisait encore probablement sentir. Signalons aussi que le terme “neuroleptanalgésie” décrit l’effet unique de ce mélange de médicaments; nous nous demandons s’il est justifiable de donner ce nom à une technique d’anesthésie générale. L’emploi de l’innovar dans le cadre du présent concept de l’anesthésie nous a donné des résultats prometteurs; il faudrait continuer de l’employer de façon régulière.
Article PDF
Similar content being viewed by others
References
Jansen, P. A. J. Vegleichende pharmakologische Daten über sechs neue basische 4-butyro-phenone Derivative. Arzneimittel-Forsch,11: 819 (1961).
DeCastro, J. &Mundeleer, P. Die Neuroleptanalgesie. Anaesthesist12: 10 (1962),
Nielssen, E. &Janssen, P. Neurolept Analgesia, an Alternative to General Anaesthesia. Acta anaesth, scandinav.5: 85 (1961).
Nielssen, E. Origin and Rationale of Neurolept Analgesia. Anesthesiology24: 267 (1963).
Henschel, W. F. An Introduction to Neurolept Analgesia, Symposium of Neurolept Analgesia, Brennen, Germany,, February, 1963. Die Neuroleptanalgesie, Springer Verlag (in preparation). Abstracts: Anaesthesist14: 21 (1965).
Dobkin, A. B.;Israel, J. A.; &Byles, R. H. Innovan-N2O Anaesthesia in Normal Man. Canad. Anaesth. Soc. J.11: 41 (1964).
Swerdlow, M. &Foldes, F. F. Narcotics and Narcotic Antagonists. Chapter 7: Supplementation of Anaesthesia. Springfield: C. C.Thomas (1964).
Steinhaus, J. E. &Howland, D. E. Intravenously Administered Lidocaine as a Supplement to Nitrous-Oxide-Thiabarbiturate Anaesthesia. Anesth. & Analg.37: 40 (1953).
Gray, C. T. &Riding, J. E. Anaesthesia for Mitral Valvotomy: The Evaluation of a Technique. Anaesthesia12: 129 (1957).
Holderness, M. C.;Chase, P. E.; &Dripps, R. D. A Narcotic Analgesic and Butyro-phenone with Nitrous Oxide for General Anaesthesia. Apiesthesiology24: 336 (1963).
Corssen, G.;Domino, E. F.; &Sweet, R. B. Neurolept Analgesia and Anaesthesia. Anesth. & Analg.43: 748 (1964).
Carignan, G.;Keeri-Szanto, M.;Lavallee, J. P.; &Lepfage, C. Innovar, First Experi-ence with a New Intravenous Anaesthetic in a Teaching Hospital. Anesth. & Analg.43: 560 (1964).
Helrich, M. &Gold, M. J. Circulatory Compensation to Tilt following Analgesic Drugs. Acta anaesth. scandinav. Suppl.XV: 97 (1964).
Bona, G.;Koch, G.; &Vandeklinden, G. The Post-Operative Course after Neurolept Analgesia. Acta anaesth. scandinav.9: 21 (1965).
Dobkin, A. B. &Lee, P. K. Y. Neuroleptanalgesics: 1. Effect of Droperidol, Fentanyl, Innovar, Benzquinamide, and Pentazocine on the Duration of Thiopental-Induced Sleep in Dogs. Canad. Anaesth. Soc. J.,12: 34 (1965).
Nickerson, M. Drug Therapy in Shock, Pathogenesis and Therapy. Berlin: Springer Verlag (1962).
Bohmert, F. &Osten, H. Untersuchungen über die Post-Operative Ventilation nach Eingriffen in Neuroleptanalgesie (Abstract), Anaesthesin14: 22 (1965).
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Spoerel, W.E., Chan, W.S. Innovar in surgical anaesthesia. Can. Anaes. Soc. J. 12, 622–633 (1965). https://doi.org/10.1007/BF03004423
Issue Date:
DOI: https://doi.org/10.1007/BF03004423