
Résumé
Introduction
Les tumeurs stromales (GIST pour gastrointestinal stromal tumors) sont les tumeurs conjonctives les plus fréquentes du tube digestif. Elles s’intègrent désormais dans un cadre nosologique précis défini par la positivité au CD117 en immunohistochimie. Nous rapportons et analysons une série de 17 GIST opérées à la Clinique chirurgicale « A » (Rabat, Maroc) entre mars 1999 et mars 2005.
Matériel et méthodes
Nous avons inclus rétrospectivement les GIST confirmées à l’examen histologique ayant comporté obligatoirement une étude immunohistochimique. Les données démographiques, cliniques, histologiques et thérapeutiques des patients ont été analysées.
Résultats
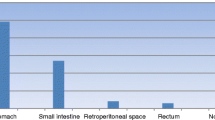
Nous avons colligé 17 cas de GIST, 8 hommes et 9 femmes. L’âge moyen était de 57 ans (extrêmes: 20–75 ans). Les localisations tumorales étaient l’estomac (n = 12) et l’intestin grêle (n = 3) puis l’œsophage (n = 1) et le rectum (n = 1). Chez 16 patients, le traitement à visée curative a consisté en une résection chirurgicale de première intention, adaptée à la localisation tumorale, sans curage ganglionnaire systématique, avec une métastasectomie hépatique dans un cas. La tumeur a été jugée inextirpable à l’exploration chirurgicale chez une patiente. La résection tumorale a été réalisée par voie cœlioscopique dans un cas. La mortalité opératoire était nulle. Les suites opératoires immédiates étaient simples à l’exception d’une éviscération libre traitée au onzième jour postopératoire. Le délai moyen de suivi était de 9 mois (extrêmes : 1–40 mois). Huit patients étaient vivants sans récidive. Une patiente ayant développé, après 8 mois des métastases hépatiques et péritonéales a été traitée par imatinib avec une régression des lésions. Un patient en récidive locale (œsophage) est décédé après 17 mois de survie globale. Sept patients ont été perdus de vue dont un ayant développé des métastases hépatiques.
Conclusion
Le potentiel évolutif de ces tumeurs reste difficile à évaluer, faute de critères histopronostiques fiables. Le devenir au long cours de nos patients opérés pour GIST doit faire l’objet d’une évaluation rapprochée et régulière en vue d’un dépistage précoce des récidives et pour établir dans un cadre prospectif les facteurs prédictifs de récidive. La chirurgie large et complète reste, dans les régions du monde où l’imatinib ne peut être distribué, la seule arme thérapeutique efficace.
Summary
Gastrointestinal stromal tumors (GIST) are the most common mesenchymal tumors of the digestive tract, now defined by the immunohistochemical expression of CD117. We report 17 cases of GIST operated between March 1999 and March 2005 in The Clinique chirurgicale « A » of Rabat (Morocco).
Methods
we have retrospectively included GIST confirmed by histopathological and immunohistochemical examination. Demographic, clinical, pathological and treatment data were analysed.
Results
seventeen patients with GIST were operated: 8 men and 9 women. The mean age was 57 years (20–75). Tumours were located in the stomach (n = 12), small intestine (n = 3), oesophagus (n = 1) and rectum (n = 1). Sixteen patients underwent a curative resection adapted to the location, without systematic lymphadenectomy. A patient underwent a hepatic metastasectomy. Resection was not possible in one patient. The mean follow-up was 9 months (1–40). Eight patients were living without recurrence. A patient who had developed liver and peritoneum metastasis was treated by imatinib with good result. A patient operated for oesophagus GIST developed a local recurrence and died 17 months after operation. Seven patients were not followed up, one with liver metastasis.
Conclusion
GIST evolution is hard to predict. Close follow-up of our patients would help us to identify and treat recurrence earlier and determine local patterns of tumour recurrence. Complete and wide surgical resection remains the only efficient treatment in regions where imatinib is not available.
Similar content being viewed by others

Références
Lecesne A. Tumeurs stromales en 2005 : état des lieux. Post’U FMC-HGE, Paris 2, 3 Avril 2005: 105–15.
Bedossa P. Les tumeurs stromales du tube digestif. Ann Pathol 1997 ; 17: 76–78.
Scoazec JY. Anatomopathologie des tumeurs stromales gastro-intestinales. La lettre de l’hépato-gastroentérologue 2003 ; hors-série : 5–9.
Scoazec JY. C-kit et tumeurs « stromales » gastrointestinales: plus qu’un nouveau marqueur. Ann. Pathol 2000; 20: 91–92.
Balaton AJ, Coindre JM, Cvitkovic F. Tumeurs stromales digestives. Gastroenterol Clin Biol 2001 ; 25: 473–82.
Le Cesne A, Boukovinas I, Terrier P, Bonvalot S, Emile JF, Vanel D, et al. Tumeurs stromales gastro-intestinales et Glivec®. 2001, Odyssée de l’oncologie. Oncoscopie 2002 ; 9: 27–32.
Pidhorecky I, Richard TC, Kraybill WG, Gibbs JF. Gastrointestinal Stromal Tumors: Current diagnosis, biologic behavior and management. Ann Surg Oncol 2000: 7 (9) : 705–12.
Landi B, Lecomte T, Cellier C. Clinical management of gastrointestinal stromal tumors. Gastroenterol Clin Biol 2004 ; 28:893–901.
Balaton AJ. Tumeurs stromales gastro-intestinales: diagnostic anatomopathologique. Oncoscopie 2002 ; 9: 23–26.
Miettinen M, Lasota J. Gastrointestinal stromal tumors — definition, clinical, histological, immunohistochemical and molecular genetic features, and differential diagnosis. Virchows Arch 2001; 438:1–12.
Ray-Coquard I, Le Cesne A, Blay JY. STI571 et tumours stromales digestives. Bull Cancer 2001, 88: 661–2.
Tuveson DA, Willis NA, Jacks T, Griffin JD, Singer S, Fletcher CD et al. STI 571 inactivation of the gastrointestinal stromale tumors c-kit oncoprotein: biological and clinical implications. Oncogene 2001 ; 20: 5054–58.
Bonvalot S. Traitement chirurgical des tumeurs stromales digestives. La lettre de l’hépato-gastroentérologue 2003 ; horssérie : 14–16.
Bonvalot S, Boige V, Apariccio T. Surgical management of gastrointestinal stromal tumors (GIST) Eur J Cancer 1999 ; 35: 1709.
Mosnier JF. Les tumeurs stromales gastro-intestinales: du gène au traitement. Hépato Gastro 2002 ; 9: 403–6.
Clère F, Carola E, Halimi C, De Gramont A, Bonvalot S, Panis Y et al. Actualités sur les tumeurs stromales gastrointestinales: à partir de sept observations de tumeurs malignes. Rev Med Interne 2002 ; 23: 499–507.
Author information
Authors and Affiliations
About this article
Cite this article
Benkabbou, A., Mohsine, R., El Malki, H.O. et al. Aspects diagnostiques et thérapeutiques des tumeurs stromales digestives. Acta Endosc 36 (Suppl 1), 441–448 (2006). https://doi.org/10.1007/BF03003388
Issue Date:
DOI: https://doi.org/10.1007/BF03003388