
Abstract
Background
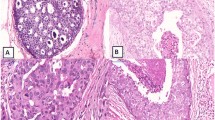
It has become common to divide ductal carcinomain situ (DCIS) of the breast into two main groups, comedo or noncomedo by tumor morphology. But noncomedo DCIS can be further stratified into several morphological patterns that exhibit several different growth patterns and most DCIS lesions have more than one pattern. In this study, DCIS elements were classified by morphological pattern and the association between predominant or recessive elements of DCIS lesions and clinicopathological findings was evaluated.
Methods
DCIS lesions from 46 patients were studied regarding the histological architectural patterns: comedo, cribriform, papillary, solid and micropapillary. The predominant architectural pattern which comprised more than 50% of the cells of the cancerous lesion was defined as the major element of the tumor and minor elements consisted of less than 50% but more than 25% of cells comprising the tumor.
Results
Of 24 tumors containing a comedo pattern as the major or minor element, 9 (38%) had microscopic intraductal spread over 2 cm and 11 (46%) had involvement of lobules, which was significantly higher than that observed in other types. Of 20 tumors containing a cribriform pattern as the major or minor element, 8 (40%) had microscopic intraductal spread over 2 cm and 9 (45%) had involvement of lobules, which was significantly higher than that seen in other types. Of 10 tumors containing a papillary type as the major or minor element, 5 (50%) had discrete multicentric lesions in the ipsilateral or contralateral breast, which was significantly higher than that seen in other types.
Conclusions
DCIS lesions containing a comedo or cribriform element are more likely to have microscopic spread and involvement of lobules and DCIS lesions containing a papillary element are likely to be multicentric, whether the pattern are predominant in the tumor or not.
Similar content being viewed by others


Abbreviations
- DCIS:
-
Ductal carcinomain situ
References
Lennington WJ, Jensen RA, Dalton LW,et al: Ductal carcinoma in situ of the breast: heterogeneity of individual lesions.Cancer 73: 118–124, 1994.
Patchefsky AS, Schwartz GF, Finkelstein SD,et al: Heterogeneity of intraductal carcinoma of the breast.Cancer 63: 731–741, 1989.
McDivitt RW, Stewart FW, Berg JW: Tumor of the breast. In: Harlan I, Feminger MD eds, Atras of Tumor Pathology, Armed Forces Institute of Pathology, Washington DC, ppl33–137, 1986.
The Consensus Conference Committee: Consensus conference on the classification of ductal carcinoma in situ.Cancer 80: 1798–1802, 1997.
Lagios MD, Westdahl PR,et al: The concept and implications of multicentricity in breast carcinoma.Pathol Ann 16: 83–102, 1981–9.
Lagios MD, Margolin FR, Westdahl PR,et al: Mammographically detected duct carcinoma in situ: Frequency of local recurrence following tylectomy and prognostic effect of nuclear grade on local recurrence.Cancer 63: 618–624, 1989.
Lagios MD, Westdahl PR, Margolin FR,et al: Duct carcinoma in situ: relationship of extent of noninvasive disease to the frequency of occult invasion, multicentricity, lymph node metastases, and short-term treatment failures.Cancer 50: 1309–1314, 1982.
Silverstein MJ, Cohlan BF, Gierson ED,et al: Duct carcinoma in situ: 227 cases without microinvasion.Eur J Cancer 28: 630–634, 1992.
Japanese Breast Cancer Society: General Rules for Clinical and Pathological Recording of Breast Cancer, 12the ed, Kanehara Publications, Tokyo, 1996 (in Japanese).
Noguchi M, Tsugawa K, Taniya T,et al: The outcome of patients with breast cancer who underwent breast conserving treatment with or without immediate volume replacement with autogenous tissue.Breast Cancer 6: 43–50, 1999.
Silverstein MJ, Waisman JR, Gamagami P,et al: Intraductal carcinoma of the breast (208 cases): Clinical factors influencing treatment choice.Cancer 66: 102–108, 1990.
Bur ME, Zimarowski ML, Schnitt SJ: Estrogen receptor immunohistochemistry in carcinoma in situ of the breast.Cancer 69: 1174–1184, 1992.
Schwartz GF, Finkel GC, Garcia JC,et al: Subclinical ductal carcinoma in situ of the breast. Treatment by local excision and surveillance alone.Cancer 70: 2468–2474, 1992.
Solin LJ, Recht A, Fourquet A,et al: Ten-year results of breast conserving surgery and definitive irradiation for intraductal carcinoma (ductal carcinoma in situ) of the breast.Cancer 68: 2337–2344, 1991.
Author information
Authors and Affiliations
Corresponding author
Additional information
Reprint requests to Hideyuki Ajisaka, Department of Surgery II, School of Medicine, Kanazawa University, Takara-machi 13-1, Kanazawa 920-0934, Japan.
About this article
Cite this article
Ajisaka, H., Tsugawa, K., Noguchi, M. et al. Histological subtypes of ductal carcinomain situ of the breast. Breast Cancer 9, 55–61 (2002). https://doi.org/10.1007/BF02967548
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02967548