
Abstract
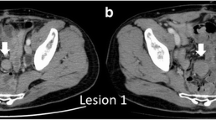
Abdominal masses, “desmoid tumors,” occur in approximately 4% of patients with Garnder's Syndrome, usually 1–3 years after total colectomy. Histologic sections usually resemble those of an infiltrating fibrous tumor, a desmoid lesion. The radiographic pattern may be similar to any diffuse abdominal retroperitoneal tumor, metastatic disease, lymphoma, or possibly retractile mesenteritis. The clinical setting usually differentiates these entities.
Similar content being viewed by others

References
Gardner EJ: Follow-up study of a family group exhibiting dominant inheritance for a syndrome including intestinal polyps, osteomas, fibromas and epidermoid cysts.Am J Hum Genet 14: 376–390, 1962
Garlin RJ, Chaudhry AP: Multiple osteomatosis, fibromas, lipomas and fibrosarcomas of the skin and mesentery, epidermoid inclusion cysts of the skin, leiomyoma and multiple intestinal polyposis.N Engl J Med 263: 1151–1158, 1960
Simpson RD, Harrison EG, Mayo CW: Mesenteric fibromatosis in familial polyposis. A variant of Gardner's Syndrome.Cancer 17: 526–534, 1964
Gardner EJ, Richards RC: Multiple cutaneous and subcutaneous lesions occurring simultaneously with hereditary polyposis and osteomatosis.Am J Hum Genet 5: 139–147, 1953
O'Brien JP, Wels P: Synchronosis occurrence of benign fibrous tissue neoplasia in hereditary adenosis of colon and rectum.NY J Med 55: 1877–1880, 1955
Miller RH, Sweet RH: Multiple polyposis of colon.Ann Surg 105: 511–515, 1930
Pugh, HL, Nesselrod TP: Multiple polypoid disease of colon and rectum.Ann Surg 121: 88–99, 1955
Gumpel RC, Carballo JD: New concept of familial adenomatosis.Ann Intern Med 45: 1045–1058, 1956
Gordon WC, Rasf MD, Whelan TJ: Gardner's Syndrome.Ann Surg 155: 538–542, 1962
Smith WG: Multiple polyposis, Gardner's Syndrome, and desmoid tumors.Dis Colon Rectum 1: 323–332, 1958
Anderson WAD:Pathology, St Louis CV Mosby, 1971, p 567
Pathologic Basis of Disease. Edited by SL Robbin. Philadelphia, WB Saunders, 1974, pp. 158 and 1478
Asch RD, Kahn LI, Freck RS: Obstruction of small intestine due to retractile mesenteritis.Gastroenterology 54: 594–598. 1968
Dineen J, Asch T, Pearce JM: Retroperitoneal fibrosis.Radiology 75: 380–390, 1960
Graham JR, Subry HI, LeCompte DR, Sadowsky NL: Fibrotic disorders associated with methysergide treatment for headache.N Engl J Med 274: 359–368, 1966
Hughes ESR, Hueston JT: Desmoid tumors in familial polyposis of the colon.Austr NZ J Surg 30: 131–139, 1960
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Menuck, L.S. Abdominal desmoid masses in Gardner's syndrome. Gastrointest Radiol 1, 81–84 (1976). https://doi.org/10.1007/BF02256345
Issue Date:
DOI: https://doi.org/10.1007/BF02256345