
Abstract
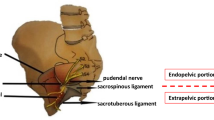
PURPOSE: Pudendal neuralgia caused by nerve compression may be improved by surgical decompression of the pudendal nerve. This study was undertaken to determine if clinical symptoms, electrophysiological investigations, and the efficacy of preoperative pudendal nerve blocks could be used to predict the efficacy of surgery. METHODS: Twelve consecutive patients complaining of anal pain, genital pain, or both, exacerbated in the sitting position and unsuccessfully treated by analgesic drugs before referral were studied. In these 12 patients decompression of the pudendal nerve was performed after unsuccessful CT-guided injection of corticosteroids in the pudendal nerve at the ischial spine or after pain relapse following successful injections. Nineteen nerves were decompressed by surgery, and the compressed area was located between the sacrospinal and sacrotuberal ligaments for 18 nerves. RESULTS: Three months after surgery, four patients were totally relieved, and three were only partially improved. After 21 months of follow-up, three patients were cured, one was slightly improved, and eight remained in pain. In the three patients cured by surgery, pain completely disappeared for at least two weeks after a nerve block repeated twice before surgery, whereas pain relief was observed in only one of the nine other patients (P=0.018). None of the three patients cured by surgery were being treated for depression, whereas six of the nine remaining patients were receiving antidepressants or were followed by a psychiatrist (P=0.09). Results of surgery did not depend on other preoperative clinical or electrophysiological data. CONCLUSIONS: This preliminary study suggests that complete disappearance of pain for at least two weeks after a nerve block repeated twice before surgery may be the best criterion to predict success. Based on this criterion, surgery would have been performed in four patients in this study, of whom three would have been cured.
Similar content being viewed by others


References
Boisson J, Debbasch L, Bensaude A. Les algies anorectales essentielles. Arch Fr Mal Appar Dig 1966;55:3–24.
Neill ME, Swash M. Chronic perianal pain: an unsolved problem. J R Soc Med 1982;75:96–101.
Swash M. Chronic perianal pain. In: Henry MM, Swash M, eds. Coloproctology and the pelvic floor. Pathophysiology and management. London: Butterworths, 1985:388–92.
Ger GC, Wexner SD, Jorge JM,et al. Evaluation and treatment of chronic intractable rectal pain, a frustrating endeavor. Dis Colon Rectum 1993;36:139–45.
Amarenco G, Lanoe Y, Ghnassia RT, Goudal H, Perrigot M. Syndrome du canal d'Alcock et névralgie périnéale. Rev Neurol (Paris) 1988;144:523–6.
Shafik A. Pudendal canal syndrome: description of a new syndrome and its treatment. Report of seven cases. Coloproctology 1991;13:102–9.
Labat JJ, Robert R, Bensigor M, Buzelin JM. Les névralgies du nerf pudendal (honteux interne). Considérations anatomo-cliniques et perspectives thérapeutiques. J Urol (Paris) 1990;96:239–44.
Amarenco G, Savatovsky I, Budet C, Perrigot M. Névralgies périnéales et syndrome du canal d'Alcock. Ann Urol (Paris) 1989;23:488–92.
Correas JM, Belin X, Amarenco G, Budet C. Infiltration scano-guidée dans le syndrome du canal d'Alcock chronique. Rev Imag Med 1990;2:547–9.
Bensigor-le Henaff M, Labat JJ, Robert R, Lajat Y, Papon M. Douleur périnéale et souffrance des nerfs honteux internes. Doul Analg 1990;3:99–101.
Schmidt RA. Technique of pudendal nerve localizaton for block or stimulation. J Urol 1989;142:1528–31.
Shafik A. The posterior approach in the treatment of pudendal canal syndrome. Coloproctology 1992;14:310–5.
Robert R, Labat JJ, Bensigor M,et al. Bases anatomiques de la chirurgie du nerf pudendal. Conséquences thérapeutiques dans certaines algies périnéales. Lyon Chir 1993;89:183–7.
Robert R, Brunet C, Faure A,et al. La chirurgie du nerf pudendal lors de certaines algies périnéales: évolution et résultats. Chirurgie 1993–1994;119:535–9.
Robert R, Labat JJ, Lehur PAet al. Réflexions cliniques, neurophysiologiques et thérapeutiques à partir de données anatomiques sur le nerf pudendal (honteux interne) lors de certaines algies périnéales. Chirurgie 1989;115:515–20.
Bensigor-le Henaff M, Labat JJ, Robert R, Lajat Y, Papon M. Douleur périnéale et souffrance des nerfs honteux internes. Agressologie 1991;32:277–9.
Snooks SJ, Swash M. Nerve stimulation techniques, pudendal nerve terminal motor latency, and spinal stimulation. In: Henry MM, Swash M, Eds. Coloproctology and the pelvic floor. Pathophysiology and management. London: Butterworths, 1985:112–25.
Swash M, Snooks SJ. Electromyography in pelvic floor disorders. In: Henry MM, Swash M, eds. Coloproctology and the pelvic floor. Pathophysiology and management. London: Butterworths, 1985:88–103.
Sangwan YP, Coller JA, Barrett MS, Murray JJ, Roberts PL, Schoetz DJ Jr. Unilateral pudendal neuropathy: significance and implications. Dis Colon Rectum 1996;39:249–51.
Ducrotte P, Rodomanska B, Weber J,et al. Colonic transit time of radiopaque markers and rectoanal manometry in patients complaining of constipation. Dis Colon Rectum 1986;29:630–4.
Touchais JY, Ducrotte O, Weber J,et al. Relationship between results of radiological pelvic floor study and anorectal manometry in patients consulting for constipation. Int J Colorect Dis 1988;3:53–8.
Shafik A. Pudendal canal decompression for the treatment of fecal incontinence in complete rectal prolapse. Am Surg 1996;62:339–43.
McKay M. Vulvodynia. Diagnostic patterns. Dermatol Clin 1992;10:423–33.
Turner MLC, Marinoff SC. Pudendal neuralgia. Am J Obstet Gynecol 1991;165:1233–6.
Hagen NA. Sharp, shooting neuropathic pain in the rectum or genitals: pudendal neuralgia. J Pain Symptom Manage 1993;8:496–501.
Magni G, de Bertolini C, Dodi G, Infantino A. Psychological findings in chronic anal pain. Psychopathology 1986;19:170–4.
Henry C, Guenther F, Guex P, Bogousslavsky J, Regli F. Douleurs ano-génitales et périnéales chroniques. Caractéristiques cliniques et psychopathologiques d'un syndrome. Rev Med Suisse Romande 1991;111:27–32.
Author information
Authors and Affiliations
About this article
Cite this article
Mauillon, J., Thoumas, D., Leroi, A.M. et al. Results of pudendal nerve neurolysis-transposition in twelve patients suffering from pudendal neuralgia. Dis Colon Rectum 42, 186–192 (1999). https://doi.org/10.1007/BF02237125
Issue Date:
DOI: https://doi.org/10.1007/BF02237125